
Patient Support Hub Programs: An End-to-End Guide
[Revised April 30, 2026]
Executive Summary
Patient support hub programs have become a central element of modern specialty-pharma operations, coordinating a patient’s journey from diagnosis to therapy. These “hubs” serve as single points of contact for referrals, insurance navigation, financial assistance, clinical support, and data management. Their rise has been driven by the explosive growth of specialty medications – now nearly half of U.S. prescription drug spending ([1]) – and the complexity and cost of modern therapies ([1]) ([2]). Hub programs may be operated by pharmaceutical manufacturers themselves or more commonly by third-party “hub providers” (e.g. Accredo, Sonexus, TrialCard, Eversana) under contract.
Architecturally, hub systems integrate diverse technologies and platforms ([3], telephony, web portals, EHR interfaces and data warehouses) to process patient referrals, authenticate benefits, secure prior authorizations, manage copay and charitable programs, coordinate shipments and pharmacies, and compile reporting data ([4]) ([5]). Data flows continuously between healthcare providers (HCPs), patients, payers, specialty pharmacies, and manufacturers (often via data aggregators) to streamline access and maximize adherence ([6]) ([7]). These data flows must be carefully controlled to maintain HIPAA and GDPR privacy compliance (requiring explicit patient consent for non-treatment uses of PHI ([8]) ([9])) and to avoid regulatory risks (e.g. Anti-Kickback fears in subsidizing copays) ([10]) ([11]).
Hub programs have measurably improved patient access and outcomes: systematic reviews show patient support initiatives significantly boost medication adherence and patient satisfaction ([12]). For example, one 2025 case study reported that deploying an integrated digital hub portal (with broad e-payor connectivity for benefits verification and ePrior-Auth) dramatically raised physician confidence and accelerated therapy starts ([13]) ([14]). Industry experts note that “end-to-end” hub solutions yield better patient experiences and outcomes by providing a single coordinated journey through enrollment, support, dispensing and follow-up ([15]).
This report provides a detailed examination of patient support hub programs end-to-end: tracing the historical evolution and current landscape; dissecting program architectures, data flows, and technology; outlining enrollment, benefits and fulfillment processes; analyzing regulatory and compliance issues; and exploring future directions. It draws on industry data (e.g. that manufacturers spent $$18.7$ billion on co-pay assistance in 2022, with industry analyses estimating spend exceeded $$23$ billion by 2024 as specialty drug volumes climbed ([10])), professional analyses, expert interviews, case studies, and peer-reviewed research to offer a comprehensive view. The conclusion highlights implications for stakeholders and forecasts emerging trends in hub-based patient support.
Introduction and Background
Patient support hub programs first emerged in the early 2000s in response to the growing specialty pharmacy sector. Specialty therapeutics (e.g. biologics for cancer, multiple sclerosis, rheumatology and rare diseases) often require complex handling, high-custody management and intensive patient support. By 2009, specialty drugs – though prescribed to a relatively small patient population – accounted for over $$21$ billion of U.S. pharmaceutical sales ([16]). These products are typically very expensive, have complicated reimbursement pathways, and demand careful patient education and adherence management ([17]) ([18]). As one industry whitepaper observed, these high-cost drugs “often necessitate a high level of patient support” and pose manifold challenges to physicians, patients, payers, pharmacies and manufacturers ([19]) ([20]).
Specialty drug manufacturers found that merely shipping products through a distribution channel was insufficient to ensure patient access and adherence. Coordination gaps – from prescription writing to benefit coverage to drug delivery – could lead to drop-offs where patients failed to start or continue therapy, impeding both outcomes and commercial success. The concept of a centralized “hub” arose as an integrated solution: a single point of contact where patients, providers, and pharmacies interface with the manufacturer to navigate access, finance, logistics and education ([4]) ([21]). An early 2011 industry whitepaper characterized the hub model as a way to “overcome complex challenges by serving as a single point of contact for patients and providers to access specialty drugs,” offering a broad set of services (distribution, call handling, intake/insurance verification, copay assistance, education, adherence support, registry and analytics) tailored to each therapy ([4]) ([21]). In short, the hub’s goal is “to partner with patients, physicians, pharmacies and manufacturers in managing specialty drug access from decision-to-treat to product delivery, including adherence support” ([21]).
Since those early days, hub programs have become ubiquitous for new specialty or high-cost therapies.By 2020, patient support had progressed from a “nice to have” to a “must-have” for drug launches ([1]). A 2020 Pharmaceutical Commerce report noted that specialty drugs constitute nearly half of U.S. drug spending, and that manufacturers face “dramatic” growth in new specialty approvals ([1]). The same survey (by Helio Health) found that outsourced hub providers are heavily used for inherently risky tasks – prior authorizations (PA), benefit verification (BV), reimbursement support and copay assistance – which, if mismanaged, carry regulatory and financial dangers ([22]). In practical terms, hub providers today routinely process a patient’s referral form, verify insurance benefits (often electronically), assist with PAs, enroll needy patients in bankruptcy/co-pay foundations, and arrange delivery through a preferred specialty pharmacy network ([23]) ([21]). They may also provide clinical nursing support, disease education, therapy reminders and outcome tracking.
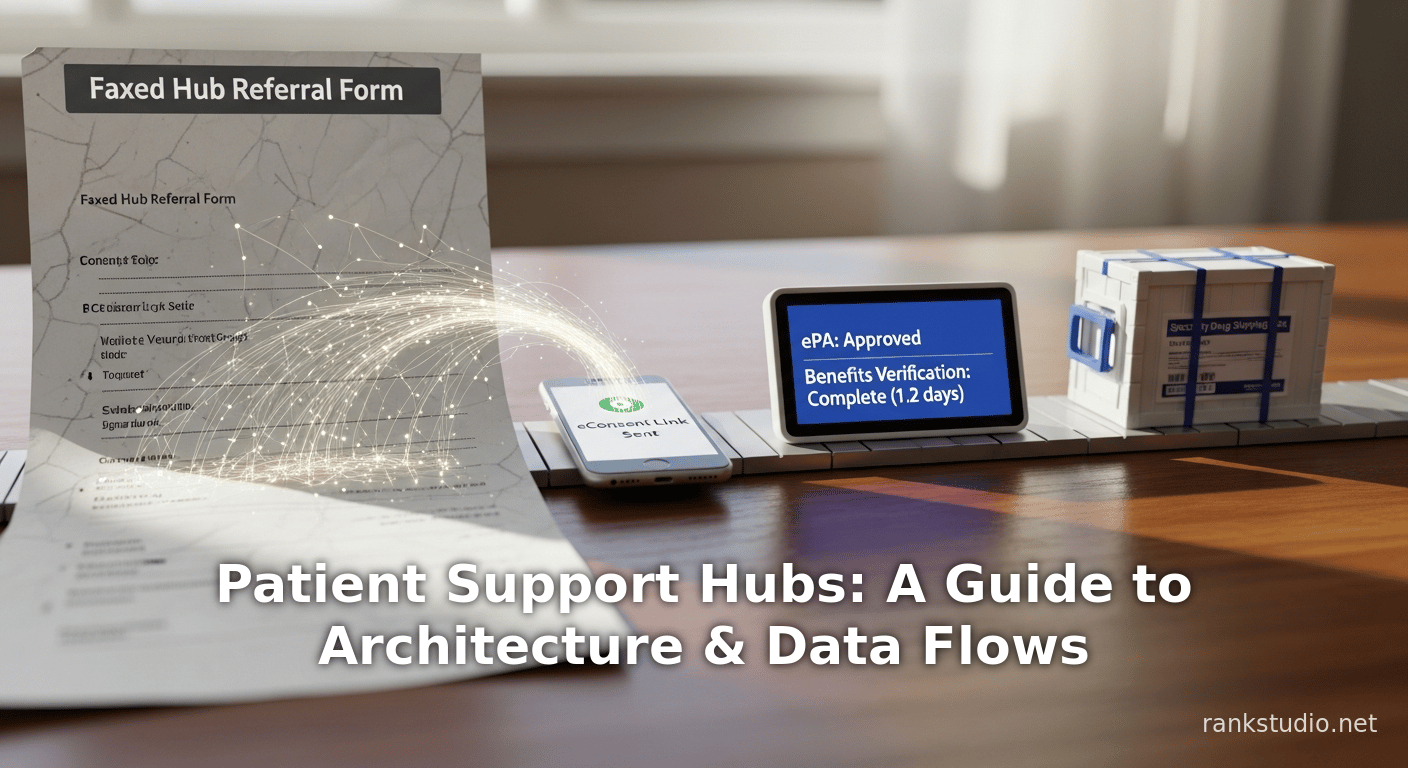
Figure 1 (below) summarizes a typical hub workflow. A prescription referral (often faxed or electronically sent by the prescriber) enters the hub intake, triggering a patient welcome process. The hub obtains patient financial and insurance data (through payer calls or e-eligibility queries) and then routes the prescription to the optimal fulfillment channel (a specialty pharmacy or infusion suite) given the patient’s coverage. If the therapy is unaffordable, the hub enrolls the patient in co-pay/copay cards, charitable assistance programs, or alternate payment support. Throughout, the hub collects and securely transmits data to the manufacturer’s analytics system, while offering portals or phone access for patients and providers to check status.
([4]) ([21]) Figure 1: Anatomy of a patient support hub program workflow. A hub receives a prescription referral (intake), then proceeds with benefits investigation, patient financial assistance (co-pay or patient assistance), referral of the prescription to the network pharmacy or site of care, and ongoing case management. Meanwhile, data about the patient’s coverage, authorization status, shipments and adherence are aggregated and reported to the manufacturer. (Source: Adapted from hub industry whitepaper ([4]) ([21]))
Over the past decade, hub services have “evolved continuously,” incorporating new technologies and expanding scope. Many modern hubs leverage sophisticated CRM platforms (such as Salesforce) and call-routing systems for multi-language support ([5]). Data aggregation has become essential: most manufacturers now engage third-party data-aggregation firms (e.g. Prometrics, LiquidHUB, ValueCentric, Shyft) that integrate feeds from all specialty pharmacies, hub systems and payer data sources ([6]). These aggregators provide dashboards giving up-to-date visibility of enrollments, dispensing, and patient outcomes to manufacturers’ field reimbursement and patient-access teams ([6]) ([7]). Meanwhile, telephonic and text-based outreach (including AI-driven chatbots) increasingly supplement human case managers to accelerate enrollment and adherence.
Looking ahead, hub programs are poised to play even larger roles in value-based care and digital health. Their strategic importance is underscored by significant industry consolidation: leading patient-support companies have acquired pharmacies, specialty data firms and digital health tools to offer true “end-to-end” solutions ([24]) ([15]). In sum, patient support “hubs” have matured from basic assistance programs into comprehensive technology-enabled platforms that coordinate the entire specialty-treatment pathway.
Evolution of Hub Programs and Patient Support
Historical Context
The hub concept originated in the early 21st century with the rise of specialty pharmaceuticals. As specialty drugs grew in number and cost, manufacturers sought to ensure patient starts and adherence by orchestrating the access process. Early hubs were often subsumed under specialty pharmacy networks or co-pay program vendors. A 2011 whitepaper by AvoidDropOff.com emphasized that specialty drugs require “significant reimbursement challenges” and “often necessitate a high level of patient support” ([19]). That paper argued a centralized program could “streamline the drug distribution, delivery, and management processes” by engaging patients, payers, providers and manufacturers in coordinated care ([20]) ([4]).
Initially, many manufacturers managed support internally or in partnership with charitable foundations. Over time, third-party hub providers emerged as specialized vendors offering modular services. For example, early entrants like TrialCard focused on copay cards while others (e.g. AVITA Medical, now Accredo) provided dispensing plus support. By 2010, manufacturers commonly tasked hubs with verifying patient insurance (Benefit Verification), assisting with PAs, enrolling patients in financial assistance, and coordinating shipment to network pharmacies ([25]) ([26]).
Through the 2010s, the hub model rapidly expanded. Between 2010 and 2020, manufacturers launched hundreds of new specialty therapies (cancer immunotherapies, high-cost autoimmune biologics, CFTR modulators, etc.), each typically accompanied by a patient support program. Hub services diversified to meet these needs: educational call centers, mobile apps, genetics testing assistance, and infusion scheduling plugins all became common offerings ([23]) ([21]). According to Pharmaceutical Commerce, by 2020 patient support was “end-to-end” for many products, even extending to clinical trial patients and sales rep support ([27]). Market data in 2020 showed specialty drugs approaching 50% of U.S. drug spend ([1]), underscoring hub programs’ importance for ensuring that high-stakes treatments actually reach patients.
The Role of Digital and Integration
A key trend in hub evolution is digitization. Automation and analytics are now a focus: 2019–2025 saw a surge in integrations with e-prescribing networks, payer portals and EHRs. For instance, Surescripts (the national e-prescribing network) launched Specialty Patient Enrollment and gateway services that allow hubs and pharmacies to electronically populate referral forms, retrieve patient clinical data and even automate prior authorizations ([28]) ([29]). These innovations aim to shave days off the start-of-care timeline. Industry surveys report that specialty approvals often took 7–10 business days historically, largely due to paperwork; new tech has begun to cut that to 1–2 days by automating PA requests and benefit checks ([28]) ([30]).
Similarly, mobile and web portals have proliferated. Many hubs now offer secure HCP portals or patient apps for referral status and education, and some pharma field reimbursement teams rely on consolidated dashboards for multi-brand data ([31]) ([32]). Electronic systems now capture patient consent, too: instead of paper fax consents, new eConsent platforms enable patients to sign digitally via email or text within minutes of enrollment ([33]) ([34]).
Industry consolidation has kept pace: several major hub providers have been acquired or merged into one-stop-shop companies. For example, TrialCard (rebranded as Mercalis in 2023 after merging with Trio Health) acquired specialized pharmacies (PC Scripts, in 2018) and mobile health firms to bundle services, and continued expanding analytics capabilities through 2025 ([24]). Eversana (a conglomerate of distribution, channel, and patient services) added HEOR and field sales firms to its portfolio, touting a seamless “integrated solution” for small-to-mid-size pharma ([35]) ([36]). These trends toward “one-stop” services reflect manufacturers’ desire for a single accountable partner covering every touchpoint of the patient journey. In March 2020, TrialCard’s CCO summarized this ethos: “End-to-end solutions provide benefits to the pharma sponsor as well as to the patient… one point of contact for the pharma company, and the patient has a better experience… The better experience from this can result in better outcomes” ([15]).
Hub Program Models and Architectures
Hub programs today exhibit a variety of operational models depending on manufacturer needs, patient population, and therapeutic context ([25]) ([37]). The major variables include the scope of services, whether the hub is mandatory or optional, the staffing model (transactional vs. dedicated support), and the integration depth with pharmacies. Table 1 below summarizes common hub model types.
| Feature | Full-Service Hub | Hub-Lite | Hybrid / Dedicated Programs |
|---|---|---|---|
| Scope of services | Offers comprehensive services: full intake, data entry, BI/BV, PA, copay and financial-assistance management, nursing/case management, education, adherence programs, REMS compliance, data reporting. Acts as central coordinator for all patient support. ([38]) ([21]) | Provides core intake and light support: collects referral, does basic benefit check and triage; may handle calls and light PAP qualifying; largely routes patients to specialty pharmacies to handle advanced tasks. Advanced services (complex PA, in-depth adherence) are offloaded to downstream partners. ([39]) ([40]) | Often used for rare or low-volume therapies. The manufacturer or hub dedicates a small team (FTEs) to one product, providing high-touch case management. May insource some functions (e.g. field calls by manufacturer). Combines elements of full-service scope with deep product/disease expertise. Example: dedicated cell/gene therapy hubs with 24/7 support ([41]) ([42]). |
| Pharmacy network | Usually limited network of specialty pharmacies mandated by manufacturer. All prescriptions flow through hub for benefit optimization and consolidated data capture. ([21]) ([43]) | Typically broad or open network. Patient may choose from multiple pharmacies. Hub mainly directs prescription to a suitable pharmacy but does not enforce network. This “non-mandatory” model is common in oncology to allow buy-and-bill or preferred pharmacy. Requires careful tracking to avoid lost referrals ([44]) ([45]). | Mix of models: some hybrids mandate core network for certain tasks while otherwise optional. For a rare drug, even if network is small, all cases may be routed through hub by design because off-label or limited providers are involved ([41]) ([42]). |
| Technology | Extensive IT integration: custom or enterprise CRM platforms, telephony systems, patient/HCP portals, e-forms, data warehouses. Emphasis on analytics dashboards and EHR/PBM connectivity. Often uses data aggregators for centralized insight ([6]) ([7]). | Lighter IT: mostly web forms or simple intake portals. Uses basic telephony/call center and email. Less automation on benefit checking; may send referrals via fax/email to pharmacies. Limited dashboard/reporting. | Can vary: some hybrids build own integrated systems for FTE teams; others (small product, big company) may allow the manufacturer’s internal team to manage via shared tools. Technology often complements the dedicated team (for example, a cell/gene hub may employ a specialized shipment-tracking system). |
| Staffing / Pricing | Typically transactional. The hub has large pooled call centers and payer-verification teams serving many programs; manufacturer pays per service (e.g. per PA, per call). Providers use temp staffing for volume swings. Examples include Sonexus, Lash, RxCrossroads ([46]). | Transactional or hybrid. The same vendor may handle multiple brands and offer limited tracking. Fees often per referral or per achievement. Minimal FTE overhead since manufacturer handles escalated care, or pharmacy takes up slack. | Dedicated model. Hub (or manufacturer) staffs a small team of employees/fellows to that product exclusively. Manufacturer often pays a flat FTE fee. Smaller hub vendors (like RareMed Solutions) specialize in such programs with deep disease knowledge ([47]). |
Table 1: Common hub program models and characteristics.
Full-service hubs (the “gray” vs “white” bag integrated models ([48])) seek to maximize efficiency and data capture by requiring nearly all prescriptions to pass through the hub. In a full-service program, the hub not only does basic insurance checks but also aggressively pursues authorization approvals, processes copay coupons or cash coupons, conducts patient education/welcome calls, and even arranges the dispensing at a chosen pharmacy. The advantage is consistency: manufacturers get uniform messaging and uniform data (e.g. precisely which pharmacy filled, how long PA took, etc.) ([21]) ([43]). For example, with mandatory hubs, the hub can “police the prescription process” – confirming the first fill and ensuring refills go to the best pharmacy from a coverage perspective ([21]).
In contrast, hub-lite models are emerging, especially for drugs under the pharmacy benefit. As of 2020, a hub-lite might simply scan intake referral forms into the hub system, perform an electronic benefit eligibility check, then auto-route the prescription to a network pharmacy ([39]). Manual intervention is minimal: if the patient can pay or has appropriate insurance, the hub’s job is largely done after confirming basic eligibility. The specialty pharmacy network then handles PAs or advanced support. Some hub-lite programs still provide a call center and patient assistance enrollment, but leave complex adherence programs or nursing support to others ([39]) ([40]).
Manufacturers also choose between mandatory vs. non-mandatory networks. A mandatory hub means all patient referrals must go through the hub (often because manufacturer wants control of the process). This guarantees full visibility of all patients and aggregated payer data. By contrast, optional or non-mandatory means physicians may dispense through any pharmacy. In U.S. oncology, non-mandatory is common, as hospitals prefer to bill themselves (buy-and-bill) or use local 340B pharmacies. Though convenient for HCPs, optional networks pose data-flow challenges: without strict coordination, referrals can fall outside the hub, requiring reconciliation to prevent “lost” prescriptions ([44]) ([45]). Advanced hubs build automated data feeds to track optional referrals and eliminate duplicates ([45]).
Finally, program size/dedication matters. High-volume drugs (e.g. biologic chronic therapies with thousands of patients) typically use large shared hubs with transactional pricing. In these, specialized agencies like Lash and RxCrossroads manage huge caseloads with large staff pools ([46]). By contrast, ultra-rare or first-in-class therapies might merit a dedicated mini-hub: the manufacturer or a boutique hub will hire a small team of experts steeped in that disease ([47]). These dedicated FTEs coordinate the handful of patients intimately (often at great expense) and may charge by salary instead of per-action ([47]) ([41]).
In practice, hybrid arrangements are common. For example, some cell and gene therapies use a hybrid hub, where the manufacturer directly hires specialized coordinators for patient-facing tasks, but outsources eligibility verification and distribution to a hub vendor ([42]). This model acknowledges that some functions (reimbursement calls, cold-chain logistics) scale better via an established hub, while other tasks (couriering a cryo-bag to a hospital within a critical window) might be managed by a dedicated team. Overall, the choice of model depends on therapeutic complexity, company size, and budget: as one executive put it, an integrated or hybrid hub solution can especially benefit smaller pharma companies that lack their own infrastructure ([15]).
Patient Enrollment and Consent Workflows
Central to any hub program is the patient enrollment and intake process. This process commences when a provider (hospital/clinic/pharmacy) sends a prescription or referral to the hub. Historically this was done by fax of a “Hub Referral Form,” but increasingly electronic methods (e-referral portal, secure email) are used. Once the hub receives a referral, it must “clear” the patient by obtaining required consents and verifying identity and benefits ([8]) ([9]).
Critically, patients must explicitly authorize the hub to share their protected health information (PHI) for program purposes. This cannot be assumed under the general Treatment/Payment/Operations (TPO) consent that HCPs use. Under HIPAA, disclosures of PHI for non-TPO purposes (like manufacturer analytics, marketing, or patient support services beyond basic care coordination) require a separate HIPAA authorization ([8]). As one industry guide explains: a HUB cannot simply forward pharmacy dispense data or patient contact info to the manufacturer without patient consent, because those uses are outside routine treatment or payment ([8]). Therefore, an enrollment form or web portal must include a signed HIPAA authorization that explicitly names the hub and manufacturer as data recipients, enumerates the types of PHI shared (e.g. demographics, diagnosis, insurance details), and states the purpose (“to provide support services, manage financial aid, and for data analytics”) ([9]). It must include an expiration date and explain the patient’s right to revoke consent ([9]). In practice, hubs often use multi-part forms or electronic questionnaires to capture this consent at or shortly after first contact.
Beyond HIPAA, hubs generally require program enrollment consent. This is essentially a “terms and conditions” agreement for the support program, covering the scope of services and the patient’s agreement to be contacted by the hub. For example, patients may be asked to agree that “ [he/she] can be contacted by phone, text, email, and mail about the [drug name] support program” ([49]), and that they “agree to be enrolled in [Drug] Support Program” ([50]). The reason this must be explicit is because of telemarketing rules. The Telephone Consumer Protection Act (TCPA) imposes strict limits on automated calls or texts. Under TCPA, even medication reminder texts to a patient cell phone require express written consent. As the hub training guide notes, sending an “autotext refill reminder” without consent would be illegal ([51]). Thus, enrollment often collects a separate TCPA opt-in (typically a required checkbox stating clear consent to be contacted via specified channels).
Owing to these requirements, modern hubs have improved their consent-capture processes. Many now use eConsent systems: after the welcome call, patients are sent a secure link by text or email to digitally sign the HIPAA and TCPA consent forms. This allows near-immediate completion (studies show this approach raises signed-consent rates dramatically vs. back-and-forth fax/mail) ([33]). Others have fully integrated e-referral forms with built-in consent fields to prevent missing data. But hurdles remain: many HCP offices still rely on paper workflows, so some hubs still receive incomplete forms and must follow up for missing signatures. When patients are mailed or faxed forms by the hub, turnaround can be slow, occasionally delaying therapy start.
Once consents are secured, the hub proceeds with data intake. It records the patient’s demographic details, insurance plan identifiers, diagnosis, prescribed regimen, and other relevant notes from the referral form. Many hub systems utilize relational databases keyed by patient or case ID. Some hubs maintain a “patient registry” for each drug, to track longitudinal information (e.g. outcomes, adverse events, therapy duration). Notably, a foundational task is assigning the case to the patient’s chosen network pharmacy or infusion clinic. In mandatory models, this is predetermined; in optional models, the hub may actively ask patients or providers for their preference. In all cases, the hub logs the pharmacy NPI and location to ensure the next step (fulfillment) is correctly directed.
Finally, hub intake often triggers an initial welcome call to the patient (by phone). This call achieves multiple aims: verify patient identity, confirm consent, educate about the support services, and gather missing benefit info or financial details (income, prior authorizations needed, etc.). While some low-touch programs allow enrollment without a call, most medium/high-touch hubs view the live interaction as crucial for data quality and rapport. The welcome call is usually scripted via the hub’s CRM system, which prompts the agent to enter or confirm fields and to offer services (e.g. “We see you have a Medicare Part D plan – do you need help with prior authorization?”). During this call, the hub agent also obtains details such as current pharmacy health (to match the Rx to the correct element, e.g. self-injectable vs. infusion center). The captured information then flows into the hub’s workflow management engine to guide the next steps (benefit checks, authorizations, and eventually distribution scheduling).
This entire enrollment workflow must be meticulously documented. Hub systems generate an Acknowledgment of Receipt (AOR) form or case note, confirming the patient is “cleared” for services. The case will not move forward unless there is a record that HIPAA and program consents are on file (or documented verbal consent for calls). Most hubs build validation checks into their intake software (e.g. blocking order release until a consent checkbox is marked). In summary, enrollment and consent form the foundation of hub compliance and set the stage for patient access: only with proper permission and data can the hub safely proceed to benefits investigation and fulfillment.
Benefits Investigation and Prior Authorization
Once a patient is enrolled, the hub’s next task is benefit investigation/verification (BI/BV) and prior authorization (PA) management. These steps determine how and whether the therapy is covered by the patient’s insurance plan – and if not, what alternatives exist. Delays here are a primary cause of treatment hold-ups, so hubs invest in both people and technology to streamline this.
For therapies billed under the pharmacy benefit, hubs typically initiate an eligibility check electronically. Many HUBs use integrated Benefit Investigation networks (such as CoverMyMeds, ERX Network, IntegriChain, etc.) or claims-data aggregators that can query up to 1,500+ insurers in real time ([13]) ([28]). For example, a recent case study described how an Eversana hub portal “leveraged electronic connectivity with over 1,500 payers” to confirm patients’ pharmacy and medical benefits in minutes ([13]). These electronic BV (eBV) systems often use APIs or clearinghouse connections to retrieve plan details: formulary tier status, co-pay amount, prior auth requirement, quantity limits and coverage gaps. In practice, around 90% of pharmacy-benefit verifications can be handled instantaneously via such electronic checks; for the remaining plans (perhaps 10% without APIs), the hub’s specialists call payer service lines to confirm coverage manually ([52]).
Even when coverage is verified, prior authorization forms often remain. Here again electronic solutions are displacing faxes. Major third-party tools exist: CoverMyMeds, Surescripts’ Electronic Prior Auth, and vendor-specific PA portals. These allow hub staff (or pharmacy print/submit workers) to electronically fill and submit PA requests to the insurer and even track their status. A 2020 Surescripts release highlights that embedding ePA in the pharmacy workflow accelerates approvals: specialty pharmacists with automated PA workflows “have both a clear path to prior authorization and the information they need to dispense the medication,” reducing delays ([28]) ([30]). In practical terms, some hubs integrate Surescripts or CoverMyMeds directly into their CRMs: once a referral is in the system, the hub can click-to-request PA and monitor the insurer’s response within the same platform. Transliteration of key data (patient demographics, medical codes, prior prescriptions) from the referral form into the ePA form is often automated, cutting human error.
For medical-benefit therapies (e.g. infusion drugs administered in clinics or hospitals), the process is different and more manual. Because these claims go through hospital or clinic billing, there is no simple pharmacy-style eBV. Hubs addressing medical benefits usually rely on extensive phone outreach: calling providers and insurance reps to check benefits, or gathering authorizations directly from providers’ offices. Prior authorizations for medical drugs can involve peer-to-peer appeals and extensive documentation of medical necessity. Some hubs dedicate specialized teams to handle these caseloads, which may require scoring protocols or nurse assessment. Because automation lags for medical PA, these processes inherently take longer. A hub specialist may call dozens of times per case to obtain approval; as Surescripts CEO Tom Skelton noted, the “specialty prescribing process is complex” when it spans both patient clinical data and payer rules ([53]).
An important tool for hubs is EHR connectivity and data access. Increasingly, hubs exploit networks that allow querying providers’ EHRs for patient clinical information (diagnoses, labs, etc) without manual faxing. Surescripts’ Specialty Medications Gateway is one such service, enabling pharmacies and hubs to pull patient charts automatically, reducing redundant calls ([28]). This ensures that hubs can determine, for example, which prior auth form to use or what justification narrative to provide the payer. Modern HL7-based standards (including updates to SCRIPT for Specialty Information) are further facilitating these flows ([54]).
Throughout BI/BV and PA handling, the hub updates its system with the outcomes: date of verification, plan details, authorization numbers, expiration dates, etc. Any cold-chain logistics or site scheduling is deferred until PA is obtained. In summary, benefits navigation in a hub program blends cutting-edge electronic verification with meticulous manual follow-up. As one hub case study reported, leveraging broad electronic payer connectivity and custom ePA forms led to 90%+ instant benefit responses and substantially higher first-pass PA approvals ([13]). Competitive advantage in the hub arena increasingly depends on this seamless payer-linkage: “PA and BV support are ‘table stakes’ for the patient support field,” industry experts note ([22]).
Financial Assistance and Copay Support
Specialty therapies often carry very high cost-sharing burdens, so patient financial assistance is a core function of hub programs. Depending on the patient’s situation, the hub may facilitate various financial pathways:
-
Manufacturer copay assistance (coupons cards): Many hubs administer sponsored copay card programs that cap patients’ out-of-pocket spending. The hub verifies patient insurance and then loads a predetermined copay amount onto a virtual card or issues coupons to pharmacies. This requires coordination with card processors and careful accounting. The hub tracks card usage (to avoid abuses) and integration with specialty pharmacies so the discount is applied at the point of sale.
-
Charity / foundation enrollment: If a patient has no coverage or cannot afford even subsidized copays, hubs often connect them with independent charitable assistance foundations (such as Patient Access Network Foundation, CancerCare, etc.). The hub assists with application documents and follow-ups. Some foundations require refills or income re-certification monthly, which the hub helps manage.
-
Generic/fallback bridging: Occasionally, if the prescribed drug is unavailable or not affordable, a hub may work with physicians to temporarily substitute an alternative or sample. (Regulations strictly limit offering samples, per the Prescription Drug Marketing Act, so this is infrequent.)
-
340B and buy-and-bill navigation: In hospital settings, hubs advise on 340B compliance (for safety-net hospitals) or help providers bill under medical benefit and obtain required discounts. While not a “free care” program, optimizing 340B eligibility reduces costs for providers and patients.
These assistance programs involve sensitive compliance issues. The scale of such support is massive: a 2025 government report noted that in 2022 drugmakers spent $18.7 billion on drug copayment assistance ([10]). While intended as patient aid, these subsidies have attracted regulatory scrutiny. The Department of Justice and OIG have argued that certain copay assistance programs may violate the Anti-Kickback Statute (AKS) if they effectively steer Medicare/Medicaid patients to higher-cost drugs ([10]). Indeed, a recent Fourth Circuit ruling confirmed that PAP-sponsored copay subsidies can constitute prohibited “remuneration” under AKS ([55]).
Hub programs thus incorporate legal safeguards. Hubs are careful to stipend only the patient (never the provider) and to follow industry “safeguards.” For example, OIG advisory opinions have carved out exceptions when aid is awarded without regard to the prescriber or regimen, and when independent foundations vet applicants ([56]). On the phone with patients, hub agents rarely discuss manufacturer marketing; their scripts emphasize patient need and financial eligibility criteria. Internally, hubs maintain audit logs showing foundation applications were approved based on income/diagnosis, not prescriber choice. Importantly, hub staff are typically forbidden from promising specific clinical outcome or coverage of branded drugs in exchange for signing up; such quid pro quo could breach AKS.
Another compliance dimension is the Sunshine Act (Open Payments). Typically, patient copay subsidies do not trigger Sunshine reporting, as the payment flows through a foundation or is disbursed directly to a pharmacy rather than to a covered recipient. However, manufacturers are nonetheless cautious with how they coordinate PAPs. Rarely, if hub personnel are involved in transferring free drug product, the PDMA samples provisions apply: literally providing a free sample must be done only to a physician if it’s for a patient or via a covered entity program. Some hubs operate on behalf of independently funded foundations (to obscure manufacturer ties), but OIG has signaled that orchestrated schemes could be problematic ([10]).
In practice, the hub’s financial assistance workflow is as follows: after benefits are checked, the hub determines if any copay or deductible applies. If so, the agent explains available assistance: “Based on your plan, your copay would be $X. We have a manufacturer copay card that can reduce your cost to $0 (or $10). Can I enroll you in that program?” If yes, the agent collects any necessary additional info (pharmacy NCPDP numbers, patient employment, etc.) and activates the copay card in the hub system. The system then transmits the card’s details to the specialty pharmacy so that at dispensing, the patient only pays the reduced amount. For patients in need, the agent offers to assess foundation eligibility. If income qualifies, the hub submits a foundation application packet on the patient’s behalf. Successful charity approval often takes weeks; during that time, many hubs will allow a limited bridge supply of medication (often a 30-day immediate free supply or extension of the drug until help arrives).
From a data perspective, all disbursements and approvals are logged. Hubs typically track metrics such as “percent of enrolled patients receiving copay assistance”, “mean copay offset”, and “time to first fill for PAP-supported patients”. These data feed into manufacturer reports demonstrating the hub’s value. Notably, specialized software is often used to manage PAP billing: some foundation disbursements end up being a line item on manufacturer financial reporting (as patient aid expense).
In summary, patient financial aid is integral to hub programs. While it greatly improves treatment affordability (for patients with uncovered costs it may be the only way therapy is possible), it also lies in a thorny regulatory area, requiring meticulous structuring and strong compliance controls. Hub providers invest in compliance training, legal oversight, and system flags to ensure adherence to anti-fraud laws. As one legal advisory observed, properly designed PAPs are “vital safety-net assistance,” but must be monitored to prevent undue influence on prescribing ([10]).
Fulfillment and Distribution
With benefits verified and authorizations in hand, the hub transitions to therapy fulfillment. The prescription must be dispensed through an appropriate channel, and logistics coordinated to deliver the drug to the patient in a timely, compliant fashion. This phase depends heavily on the therapy’s nature (self-injectable vs. infusion vs. inhaler) and the contractual network.
Specialty pharmacy coordination: In typical oral or self-inject injectable programs, the manufacturer designates one or more specialty pharmacies (SPs) to fill the prescription. The hub electronically or manually refers the patient to the chosen SP. In mandatory networks, this choice may be fixed; in non-mandatory networks, the hub might ask the patient’s preference (say, a local pharmacy). The hub provides the SP with the case data, including any discounts or PAP info, so the pharmacy can invoice the payer correctly. After dispensing, the SP feeds status back to the hub: many hubs receive electronic refill/dispense data (via EDI claims or direct API) feeding patient adherence tracking.
Infusion centers and clinics: For drugs administered at hospitals or infusion suites, the fulfillment is via the medical benefit channel. The hub’s role here is largely coordination: ensuring the clinic has the drug on-site when treatment is scheduled. In many cases, the manufacturer works with a specialty distributor or commercial drug wholesaler to physically ship the medication to the hospital. The hub confirms deliverables with the distributor, arranges courier (especially for time-sensitive biologics), and ensures payments are processed (often 340B or buy-and-bill billing). Because continuity is critical (missing an infusion window can destroy the drug vial), hubs may set up direct lines with the distributor’s tracking system.
White-bagging vs. brown-bagging: Some hub programs specify white-bagging (insurer ships drug to provider) or brown-bagging (patient picks up from pharmacy and brings to infusion). These affect data flows: white-bag means insurer or hub tracks shipments; brown-bag is less common due to regulatory restrictions on patients carrying meds. In white-bagging, the hub may authorize the specialty pharmacy or distributor to “fill planning” for a clinical site. The hub logs shipment dates in its database to correlate with infusion appointments.
Cold-chain and specialty logistics: Many specialty therapies are temperature-sensitive (biologics, injectables). Hubs work with specialty logistics firms. For example, a hub may contract with a 3PL (e.g. Marken, CSM) to manage cold shipments; the hub’s system holds tracking numbers and expected arrival windows. Any temperature excursion is flagged by the hub so a backup plan can be deployed. Such logistics details are often outside the hub’s software, but they rely on the hub to have standard operating procedures (SOPs) for receipt and return of product if needed.
Patient convenience services: Once medication is ready, hubs often coordinate final patient delivery. If the patient receives at home (for self-injectables), the hub may arrange overnight courier or pharmacy delivery and provide test kits (auto-injector pens, sharps containers, refrigeration packs). Tracking numbers are recorded and communicated to the patient. Many hubs now provide shipment status SMS messages (“Your injection is scheduled to arrive tomorrow”). If multiple shipments are needed (e.g., weekly injectables), the hub often schedules them out and reminds the patient to ensure doses are not missed.
After the drug is dispensed, the hub continues smaller-scale case management: refill reminders, adherence check-ins, and new support as needed. But from a data perspective, a key responsibility has been completed: the case transitions from authorization to therapy in progress.
Among specialty pharmacies and hubs, buy-and-bill remains a complicating factor. In hospital settings where doctors administer the drug (buy-and-bill), the provider typically bills the insurer directly, and the role of the hub is to support the provider in obtaining payment post-delivery. Hubs often assist buy-and-bill providers with coding, appeals, and follow-up. They may also monitor accrual: if a provider has procured a drug but not dispensed it due to denial, the hub helps resubmit or advises on next steps. However, since the provider is the payer’s counterparty, the hub’s ultimate leverage is indirect (through support and persuasion rather than direct shipments).
Chain of custody and traceability is also crucial. The Drug Supply Chain Security Act (DSCSA) in the U.S. requires end-to-end tracking of prescription medications. Hubs typically do not hold large inventories, but they interact with authorized distributors who do. The hub must ensure that any shipped product has proper DSCSA pedigree information. Modern hub software often integrates with distribution partners’ serialization tracking to verify lot numbers and authenticity at the point of dispensing. This is especially important for exclusive therapies, where failures would have major consequences.
In summary, fulfillment is where the hub’s preparatory work pays off – the therapy reaches the patient. Hubs coordinate between multiple parties (pharmacies, clinics, logistics) to make this as seamless as possible. Key performance indicators (KPIs) at this stage include “time from referral to first fill” and “fill rate” (the percentage of enrolled patients who actually receive medication). High-performing hubs drive these metrics down dramatically compared to non-coordinated processes, which otherwise could leave many patients waiting months for treatment. The quest for “speed to therapy” remains a central competitive factor in hub services, as noted in a recent industry review ([13]) ([28]).
Data Aggregation, Analytics and Reporting
Throughout enrollment, benefits, and fulfillment, vast amounts of data are collected. Sophisticated data flows are the backbone of modern hub operations, enabling parties to coordinate effectively and enabling manufacturers to derive insights. Figure 2 illustrates key data incidents and interfaces in a typical hub network.
([5]) ([6]) Figure 2: Data flow in a patient support hub program. Data originates from referrals (HCP offices electonic/paper), flows through the hub’s CRM, and further to specialty pharmacies, payers, and manufacturers. Key flows: (A) Patient referral and consent data from the provider to the hub. (B) Verification results from payers to hub; coverage and co-pay data. (C) Authorization approvals from payers back to hub. (D) Dispensing data from specialty pharmacies to data aggregators/hub. (E) Aggregated network data (claims, dates, outcomes) fed to manufacturer portals. (F) Patient-reported outcomes or adherence data reported via portal. All flows must comply with HIPAA/GDPR security and require patient consent for sharing. (Illustration not to scale.)
Hub CRM/Platform: At the center is the hub’s technology platform (often Salesforce-based or a proprietary system). This database holds each patient’s profile and status. All HCP referrals, consents, demographic data, benefit findings, PA tracking numbers, shipment details, and case notes are entered here. The platform also logs each phone call or email exchange. It generates work queues and reminders for agents (e.g. follow-up on a pending PA in 48 hours) and enforces rules (e.g. do not submit PAs before verifying insurance). Many advanced hubs integrate AI modules into the CRM – for example, automatic speech-to-text to log call content, or OCR to extract data from faxed forms, reducing manual data entry ([34]).
Payer Interfaces: Hub platforms connect to payers in several ways. For eBV and ePA, the hub’s system may connect via SFTP or API to authorization services (Actics, CoverMyMeds, EHR-integrated scripts ([57]) ([28])). These connections push patient IDs to payers and import response files. In institutional settings, hubs also track informal data (notes from PA approvers, appeals outcomes) often received by fax or upload. All results are structured in the CRM (e.g., “PA Amt Approved: $10,000 dose; expiry 6/2026”).
Specialty Pharmacy and Vendor Feeds: HUB programs rely heavily on timely dispense data. After a fill is made, specialty pharmacies send transaction level data through data aggregators. For example, an SP may transmit an HL7 or EDI claim record to the aggregator, which then normalizes and pushes it into manufacturer analytics platforms. To maintain compliance, the raw PHI (patient identifiers) is typically stripped before aggregation. The manufacturer receives deidentified counts and metrics (but see “Field Reporting” below for limited direct data sharing). Meanwhile, the hub itself may get back-case status if it hosts a portal or its CRM includes pharmacy interfaces: some hubs have direct EDI feeds from their own or partner SPs so the hub knows “patient XY got drug on date Z at pharmacy N.”
Patient and Provider Portals: Modern hubs often include portals or apps for patients and HCPs. Patients can log in to check their medication order status, access educational content, or report side effects. Data entered by patients (e.g. self-reported symptom diaries or adherence confirmations) flows back into the hub database and can be aggregated by the manufacturer. Some hubs also integrate with remote monitoring devices (for example, infusion pump logs, or smart injection pens), funneling data into patient records. For providers, HCP portals allow doctors and nurses to see referral status and to upload documents (lab results, EHR queries) directly, feeding directly into the hub’s workflow. These portals generate their own data (e.g. number of portal logins, documents uploaded) which hubs can track as performance metrics.
Data Aggregators / Analytics: A critical component in the architecture is the use of third-party data aggregators. These companies (e.g. Prometrics, LiquidHUB, Shyft) sit “above” the hub and pharmacy networks. They consume flat files or feeds (SFTP transfers, API tokens) from each network partner – hub vendors, specialty pharmacies, patient registries – and harmonize the data. The aggregator then provides a unified view to manufacturers: an integrated dashboard showing all patient activity across networks ([6]). For example, such a dashboard might display metrics by week: number of referrals, number moving to fill, average time to payer determination, copay assistance dollars disbursed. Crucially, these portals incorporate access controls: sensitive details (like patient name or PHI) are not shown to field reps. The hub uses these dashboards to benchmark performance (e.g. network-wide PA turnaround times) and to identify gaps (e.g. is a particular pharmacy lagging on refills).
Field Reimbursement Reporting: A unique data flow is to the manufacturer’s sales and field teams. As [40†L134-L142] and [42†L144-L148] note, hubs and aggregators can share limited information with field access managers and reimbursement liaisons. For example, a field access rep might see that a certain doctor’s patients tend to hit a specific formulary barrier (a particular prior auth denial). However, HIPAA forbids giving identifying patient data to sales. To navigate this, many organizations employ Patient Access Teams (PATs) – field agents not tied to sales quotas – who can view non-HIPAA data from the aggregator. Sales reps typically receive only aggregated high-level insights (e.g. “Plan X is denying this drug 40% of the time”). This controlled data sharing helps align strategy: field teams learn where to focus payer negotiations, and hubs adjust processes for problematic accounts.
Data Governance and Security: Large-scale data collection introduces privacy and security obligations. Hub and pharma IT systems must comply with HIPAA Security Rule (encryption at rest and in transit, audit logs, access controls) ([8]) ([9]). Multitenant hubs implement strict role-based access; all data exchanges use secure protocols (SFTP, HTTPS). Protected data flows (like transcripts of phone calls containing PHI) are often anonymized or only available under special request. In Europe or other regions with GDPR, patient data requires even more stringent consent and anonymization practices. Any cross-border transfers (e.g. global hubs serving multiple countries) need data processing and transfer agreements. Compliance teams at hub providers routinely audit data pipelines to ensure no violations (e.g. no PHI seen by unauthorized vendors).
Reporting and Analytics: For manufacturers, one of the hub’s most valuable outputs is analytics. Hubs regularly deliver reports on patient counts, enrollment funnel dropoff, adherence rates, and other KPIs. For example, a drug launch team might receive a weekly report summarizing: “2000 referrals received; 1800 enrolled (90%); 1500 benefit verified (83% of enrolled); 1400 PA submitted (78%); 950 approved (52%); 850 first fills dispensed (47%). Average turnaround: 2.5 days to fill.” These metrics allow identification of bottlenecks. Many hubs now use business-intelligence tools (like Tableau or Power BI) to present trends over time. For certain outcomes-based contracting, real-world outcomes data (e.g. patient adherence collected via hub calls) can be compiled by the hub for validation of performance.
In sum, data flow in a patient hub environment is rich and bidirectional. A seamless hub architecture tightly interconnects the front-end intake, telephony, and portal systems with back-end payor and pharmacy networks. The result is near real-time orchestration of the patient journey. But it also requires constant governance: each data handoff must be authorized and secure, and patient consents must explicitly cover the uses of the data (as captured in the onboarding process ([8]) ([9])). When done effectively, this data-driven model has proven to reduce delays and reveal insights that disjointed manual processes simply cannot.
Compliance and Regulatory Considerations
Hub programs operate at the nexus of healthcare delivery and industry, so they face a complex web of regulatory and compliance requirements. Ensuring legal compliance is a top priority for all stakeholders in the hub.
Privacy and Data Protection
HIPAA/HITECH (USA): In the United States, patient data handled by hubs is protected under HIPAA. The hub itself is often a “Business Associate” of the manufacturers and providers. This means the hub must implement the same safeguards as any healthcare provider or insurer – administrative, physical and technical. In practice, hubs employ encryption (at-rest and TLS in transit), secure idle-time logouts, multi-factor authentication, and regular risk assessments. Patient identifiers collected during intake are stored on HIPAA-compliant servers (often AWS or Azure clouds with BAA agreements).
As noted earlier, specific consents (HIPAA authorizations) are needed to share PHI beyond treatment/procurement. Missing a consent can invalidate data usage retroactively, so hubs typically enforce a “no data, no go” policy: no health data is processed or forwarded to manufacturers without a valid HIPAA form on file ([8]). Similarly, TCPA compliance requires audit trails showing patient opt-ins for calls/SMS, as the first hub article described ([51]).
GDPR (EU): In Europe, hub-like services (often run by pharmaceutical “PAPs” or patient service representatives) must comply with GDPR. This includes strict data minimization and the need for lawful bases of processing (usually consent or contract performance). While Europe lacks the same framework as HIPAA, GDPR imposes higher fines. Thus, pharma companies ensure contract language covers hubs’ processing of EU data, often by anonymizing data sent to global analytics. If a patient resides in the EU/UK, the hub collects consent for data uses under GDPR rules and limits cross-border transfers (e.g. via Standard Contractual Clauses). In practice, global hubs often segregate EU patient records so that only deidentified metrics leave the EEA.
Other Privacy Laws: Canada’s PIPEDA, Australia’s Privacy Act, and various state laws (e.g. CCPA/CPRA in California) may also apply when hubs handle multi-jurisdiction data. Gaining patient consent upon enrollment (as part of a global consent form) typically includes clauses permitting necessary data sharing in compliance with all relevant laws. Any data residency requirements (e.g. local data stores) are managed by configuring cloud resources regionally.
Fraud, Waste and Abuse Laws
Hubs must be vigilant against violating CMS’s anti-fraud regulations. The paramount U.S. law here is the Anti-Kickback Statute (AKS) ([58]). AKS prohibits exchanging any remuneration to induce referrals or purchases of items payable by federal healthcare programs. Copay assistance is, in effect, a form of remuneration to patients. The concern is that subsidizing copays for federally insured patients could induce them to choose one manufacturer’s drug over a generic or competitor, thereby increasing Medicare/Medicaid costs illegally ([10]).
As described in the May 2025 Congress report, OIG has taken a stricter view of copay assistance programs. In Pharmaceutical Coalition for Patient Access v. United States (4th Cir., 2025), the court upheld OIG’s determination that certain PAP co-pay programs could violate AKS, and the Supreme Court declined to review the decision in early 2026, leaving the ruling in force ([55]). Hubs must thus operate under safe harbor principles: assistance should not consider the prescriber’s choices or favor one therapy, and funding should go through independent foundations when possible ([56]). Many hubs rout patient aid through a contract pharmacy that meets OIG-approved conditions. Detailed audits are performed to ensure, for example, that assistance is only provided after the patient qualifies by income/medical need, not because of any steering by the hub or manufacturer. ([10]) ([56]).
Furthermore, the Stark Law (self-referral law) does not directly bar patient assistance, but related OIG Fraud Alerts caution that “sham” co-pay programs could implicate false claims if payers overpay because of covered individuals using more expensive drugs under PAPs ([10]). Hubs train staff to avoid any language that suggests providers should prescribe because of the financial assistance – that could risk fraud charges. If any element of the assistance might indirectly influence referral, companies seek OIG Advisory Opinions; indeed, pharma companies have requested multiple AKS advisory opinions on PAP structures ([56]).
False Claims Act (FCA): If a hub inadvertently causes a claim to be submitted under false pretenses (e.g. submitting a claim for a patient who lacked authorization, or failing to disclose in a claim a copay offset), the FCA could be triggered. Therefore, hubs monitor claims data to ensure that insurers are charged properly after assistance is applied. For example, some payers audit for instances where assistance should have been applied. Hubs must also keep precise records to defend against any overcharge allegations. Penalties under FCA can be multiples of the claim amount, so compliance controls are stringent.
PDMA (Drug Samples): Although not a typical hub issue, the Prescription Drug Marketing Act governs free samples. Hubs must ensure any trial supply given to it (rare, but possible for patient start-up) is handled per PDMA (samples only to prescribers for immediate patient use, properly documented). If a hub holds buffer stock of a drug, it must be licensed as a pharmacy or otherwise meet PDMA rules. This rarely applies to hubs that generally do not stock product but is relevant when dealing with prototype therapies.
Manufacturer Codes of Conduct: Many pharma trade groups (PhRMA, EFPIA, etc.) have voluntary codes limiting interactions. Under the PhRMA Code of Ethics, for instance, manufacturers are discouraged from providing substantial financial assistance programs outside of charitable foundations. Hubs operating directly under contract with the manufacturer must ensure their programs align with the manufacturer’s corporate compliance policies. For example, physicians should not receive anything of value from the hub; even inadvertently providing branded merchandise or hospitality to providers during hub-sponsored events could be a violation.
HIPAA Privacy (as discussed) is also a compliance domain. Hubs must sign Business Associate Agreements (BAAs) with any covered entities they work with (e.g. specialty pharmacies, clinics). All staff undergo HIPAA training. A breach (unauthorized disclosure) triggered by a hub could lead to serious fines (up to $1.5M per violation category). Therefore, hubs typically have incident response plans and encrypt all PHI. Given the sensitivity, sophisticated hubs also perform regular penetration testing and comply with HITRUST or similar frameworks where possible.
Other laws: Outside the U.S., hubs contend with bribery/range laws (e.g. EU anti-corruption directives), since offering anything of value (even assistance) to induce prescription can be seen as a form of bribery in some jurisdictions. Many French or Italian pharma compliance teams periodically review PAP/hub programs to ensure they don’t conflict with local laws on anti-kickback. Data-protection regulations (GDPR) as noted, require patient data to be used only for the stated medical purpose; hubs must destroy or anonymize data when its purpose (enrollment and service provision) is completed, unless broader consent was obtained.
In sum, compliance for hub programs is multifaceted: HIPAA, fraud/abuse, general corporate ethics, and global privacy laws. Hub vendors maintain compliance departments that embed policies into every SOP. For instance, every hub agent’s workflow is guided by critical rules (marked fields on consent forms, double-check eligibility codebooks for regulatory flags, etc.). Quarterly audits of random cases are common – an auditor will review that consents were signed, assistance was awarded per guidelines, and communications avoided any prohibited influence. Because enforcement actions against PAPs have been on the rise ([59]), hubs now operate conservatively: they often refrain from any direct marketing of a drug to enrolled patients (instead focusing on education) and keep financial assistance expenditures transparent. This conservative approach both ensures legal soundness and maintains patient trust.
Impact on Outcomes and Stakeholder Perspectives
The ultimate measure of hub programs is patient outcomes and system efficiency. Growing evidence shows that well-executed support programs can significantly improve adherence, clinical outcomes, and patient satisfaction ([12]). A 2016 systematic review found that ~66% of published Patient Support Programs reported statistically significant improvements in medication adherence, and ~64% showed better patient quality-of-life outcomes, with many noting reduced healthcare utilization ([12]). In practice, hubs report high satisfaction scores: one recent case study of a digital hub portal recorded a 9.1/10 physician satisfaction rating, citing increased confidence in reimbursement and faster access ([14]).
From the patient’s perspective, hubs aim to remove barriers. Studies of patient support show that initial enrollment hurdles (insurance confusion, fear of copays, delayed start) are the greatest drop-off points. Hubs counteract this by proactively reaching out and walking patients through paperwork, often providing emotional support. Patients generally appreciate having a single contact for questions. Of course, perceptions vary: some worry about privacy or being “marketed to,” so hubs increasingly emphasize patient advocacy and education over promotion.
Clinicians and pharmacies largely view hubs positively when they work smoothly. Phone support for PAPs, real-time insurance info, and scheduled deliveries can save providers’ staff many hours. However, frustration arises if the hub process is opaque or slow. For example, if a provider sends an Rx and does not hear back, they may feel hindered. Good hub programs manage this by offering provider portals or case reps who update the physician’s office. Specialty pharmacists, in particular, benefit from integrated systems: one should see from [51†L42-L51] that the new Surescripts tools empower them by giving clinical data “so we can focus on caring for our patients.” Pharmacies also gain from streamlined PAs – the hub essentially fronts the work so they can dispense more quickly.
Manufacturers see hubs as strategic for competitive advantage. In a market where multiple drugs may treat the same condition, a manufacturer who gets patients to therapy faster and cost-effectively gains market share. The 2020 industry report notes that hubs allow manufacturers to “control costs, build relationships, and create an environment that promotes patient compliance” ([60]) ([21]). Moreover, for launch planning, insight from hub data on insurance barriers can inform market access strategies. Manufacturers expect detailed reporting (often weekly or monthly) on refill rates, reasons for discontinuation, and even patient outcome measures when applicable. This data can feed into value-based contracting decisions, pay-for-performance models, and ongoing label expansions.
Payers have a mixed view. On one hand, hubs reduce redundant prescriptions and ensure prior auth rules are followed, which can save payers money relative to unmanaged spend. On the other hand, copay assistance subsidizes patient cost-sharing, which can inflate total drug spending. Some payers have criticized copay cards for driving up branded drug use. However, many payers appreciate hubs doing the heavy lifting on PAs and patient education – it lightens their administrative load. The interplay of payer-hub relationship varies: for example, some hubs integrate directly into payer systems (via Payer Provider Portals) so that PAs initiated by the hub feed directly into the insurer’s workflow. Others have more informal connections. In any event, hubs must manage payer queries and adhere to guidelines to maintain positive relationships.
Regulators and Advocacy groups are also stakeholders. Patient advocacy organizations generally support hub programs as means to improve access. Equity and affordability advocates, however, are attentive: they push for transparency in how programs calculate benefit and copay assistance, especially to guard against patient data being used for marketing. Regulatory bodies (e.g. CMS, OIG) monitor hub-related activities via audits and through enforcement of fraud rules, as noted above. Overall, though, unless legal stepping over occurs, hubs are widely seen as a net positive innovation for patient care coordination.
Case Studies and Examples
Digital Specialties Hub (Eversana, 2025): An illustrative example is Eversana’s 2025 case of launching a new specialty drug. The manufacturer had low initial physician adoption due to complex reimbursement. Eversana deployed a digital hub portal integrated with its ACTICS eAccess platform. The portal connected electronically to over 1,500 payers for eBV/ePA. HCP survey feedback gave the hub a 9.1/10 “ease of navigation” score ([14]). Key results: 92% of benefit verifications were completed in real-time (average <1 minute) and initial PA acceptance rates jumped by 25%. The hub also implemented a “replacement” program, providing free products to physicians if their patients switched brands. Consequently, the manufacturer saw a significant uptick in prescriptions filled and reduced time-to-first-fill by 40%. This case highlights how sophisticated connectivity (eBV/ePA) can move the needle on launch metrics ([57]) ([14]).
Oncology Hub during COVID-19 (AbbVie, 2021): In a 2021 patient-support article, AbbVie described modifications to its oncology hub amid the COVID-19 pandemic. When travel was limited, the hub expanded telehealth and home-delivery for injections ([61]). Nurses switched to video monitoring and virtual support groups. The hub also adapted formulary guidance as insurers changed policies. As a result, AbbVie reported continuity of therapy in >90% of adherent patients despite lockdowns. While not involving novel tech, this case shows agility: hubs can rapidly re-scope services (e.g. wearing PPE, staggering deliveries) when external disruptions occur ([61]).
Rare Disease Hub (RareMed Solutions): Rare diseases often demand fully customized hubs. RareMed Solutions (provider for orphan therapies) uses a homegrown “SWFT™” platform that allows real-time modifications. For example, when a new genetic test became required for plan approval, the hub quickly updated its intake script to capture this info during first patient calls ([62]). RareMed’s dedicated model charges clients by FTE, reflecting the high-touch service. They report near-zero drop-off rates: i.e. almost every referred patient is worked through to therapy, via continual phone outreach and personalized assistance (travel accommodations, mental health coordination for patients, etc.). This model contrasts sharply with high-volume hubs: it is expensive per patient but often necessary to prevent catastrophic loss in ultra-rare cases.
Specialty Pharmacy Integration: A niche example is Foundry, a specialty pharmacy that positions itself as an “inpatient” broker. On certain oncology products, Foundry acted as the hub. Incoming 340B hospital orders were rerouted to Foundry’s pharmacy inventory, which then dispensed and relabeled the vial (in compliance with state laws). Foundry managed the PA and enrollment under hub-like workflows. This integrated buy-and-bill support helped hospitals maintain 340B margins while ensuring same-day med availability. Such models illustrate hybrid hub-pharmacy roles that can emerge in verticalized systems.
International Differences: In Europe and other markets, hub-like services exist but often under different structures. For example, some EU countries use contracted third-party agencies or APBI (agent protocol by indication) networks to support complex therapies. GDPR imposes more stringent consent, so European hubs often de-identify data when sending to manufacturers. A 2022 review noted that co-pay assistance programs (even voluntary ones) have faced legal scrutiny in several EU jurisdictions under similar anti-kickback reasoning, so EU hubs are careful to channel assistance through patient charities wherever possible.
Discussion and Future Directions
As healthcare continues shifting toward value-based care and data-driven management, hub programs are likely to evolve in response:
-
Advanced Analytics and Generative AI: Hubs will increasingly apply predictive analytics to prioritize interventions. For instance, AI could flag a patient less likely to complete treatment (due to socioeconomic factors) and escalate them to specialized support. By 2025–2026, several major hub vendors (Eversana, Cardinal Health Sonexus, AssistRx) had production deployments of large-language-model agents handling intake summarization, automated PA letter drafting, and post-call summary generation. Early AI pilots are underway (as one hub executive noted, machine learning will “inevitably play a major role” in improving efficiency ([63])). AI-based OCR is now standard for auto-populating referral forms ([34]). NLP on call transcripts is now used for real-time agent assist and adverse event detection.
-
CMS Prior Authorization Mandate: The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), with key provisions effective January 2026 and full API requirements by January 2027, requires impacted payers to implement FHIR-based Prior Authorization APIs and decision turnarounds of 72 hours (urgent) and 7 days (standard). This is reshaping hub PA workflows, dramatically reducing the manual phone/fax burden that has historically defined the medical-benefit PA process.
-
Interoperability and Standards: The Surescripts and NCPDP initiatives suggest a future where specialty prescribing is fully electronic. The Specialty Patient Enrollment service promises an HL7 or FHIR form that integrates seamlessly into EHRs ([29]). By 2026 vision statements in U.S. HealthIT aim for ubiquitous FHIR-based data sharing. If hubs and EHRs both adopt FHIR Consent and Clinical Data standards, referral and coverage verification could become frictionless. Global adoption of unique patient identifiers (like NHS numbers in UK) would further streamline intake.
-
Telehealth and Remote Care: The hub’s role could expand into clinical territory. Some hubs already employ nurses who manage subcutaneous injections remotely. As digital therapeutics emerge, hubs may integrate these tools to track patient vitals or adherence through apps or connected devices. For example, a hub might provide a digital inhaler that reports usage back to the support team, who then intervene proactively.
-
Pharmacy Commerce and 340B Interaction: The growth of value-based pharmacy (e.g., at-risk PBMs like Optum’s specialty arm) may reshape how hubs coordinate with pharmacies. If specialty pharmacies internalize hubs (as some vertically integrate), hubs might become in-house arms of PBMs. Conversely, regulations like Medicare’s CoE and reimburst, shifting models, could affect hub strategies. For instance, a potential federal requirement to count copay assistance toward out-of-pocket max would alter SIS programs dramatically, forcing hubs to adapt their copay workflows. The proliferation of copay accumulator and maximizer programs (now used by a majority of large commercial plans as of 2025) has already forced hub vendors to redesign assistance disbursement logic and to offer alternative funding pathways for patients whose copay card dollars no longer count toward their deductible.
-
Globalization: As pharma globalization continues, manifold regions (Latin America, Asia, Africa) are developing their own hub-like patient assistance channels. Some companies are extending hub platforms internationally, but regulatory differences (e.g. varying data laws, import restrictions) require local adaptation. There is growing interest in harmonizing these global patient access systems, possibly via multi-country IT architectures.
-
Blockchain and Trust: One academic suggestion is using blockchain for supply chain transparency and patient consent audit trails. Though still theoretical, a blockchain-based consent ledger (immutable record of patient authorizations) could address audit concerns. Similarly, distributed ledgers might authenticate specialty drug shipments end-to-end. Such technologies could bolster trust in cooperatives of multiple stakeholders.
-
Privacy Enhancements: Post-GDPR, patient consent management systems will become more sophisticated. We may see “consent hubs” that not only obtain consents but allow patients to manage them (e.g. revoke, see how data is used). Privacy-enhancing technologies (PETs) could enable more analytics on patient outcomes without compromising identity.
-
Role in Value-Based Contracts: Patient hubs will likely integrate directly with value-based agreement infrastructure. If a drug is on outcomes-based payment terms, the hub might collect data needed to adjudicate the deal (e.g., lab results or hospitalization records). Coordinating with payers to report these metrics could become a hub-mandated function.
Notable challenges remain. Chief among them is interoperability: many providers still use faxes; complete digital integration is not universal. The availability of patient data across siloed EHR systems will constrain hubs until standards like FHIR are fully implemented. Another challenge is consent fatigue: patients often sign multiple forms, and overloading them with digital paperwork can cause drop-offs. Hubs will need to continue streamlining consent capture (perhaps through apps or single sign-on mechanisms with basic care records).
Additionally, ethical issues are emerging. Critics question whether hubs sometimes prioritize drug access over independent patient choice, particularly if patient advocacy teams subscribe to manufacturer messaging. Oversight groups urge transparency. Future regulations may tighten how PATs (patient access teams) operate, perhaps requiring clear labeling of manufacturer affiliations on communications.
Finally, technological maintenance is a constant: healthcare IT evolves rapidly, and hubs must keep pace with new payer portals, EHR upgrades, telephony standards (e.g. VoIP security), etc. Continuous investment in IT modernization is needed or hubs risk becoming bottlenecks themselves.
Conclusion
Patient support hub programs have transformed how complex therapies reach patients. They have evolved from basic call centers to integrated platforms that handle enrollment, payor navigation, fulfillment and analytics. By providing a guided, data-driven journey, hubs improve access and adherence for high-cost specialty treatments. This report detailed the multifaceted architecture of a hub: referral intake, telephony and e-routing, benefit investigation and authorization, patient assistance, logistics coordination, and data reporting. Each step involves intricate data exchanges among providers, payors, pharmacies, and manufacturers. We have also examined the regulatory landscape, noting how hubs balance patient privacy protections (HIPAA/GDPR) with healthcare fraud/abuse prohibitions (AKS/”sunshine” compliance).
The cumulative evidence is clear that well-run support hubs can raise medication adherence and patient outcomes ([12]), making them an essential component of modern specialty healthcare. However, they must navigate a complex compliance environment to maintain trust. As therapies advance (e.g. gene therapy, digital drugs), hub programs will need to adapt – becoming more technologically sophisticated while upholding patient rights and ethical standards.
In the future, hubs are poised to become even more central to the patient care ecosystem. Their data can fuel predictive analytics and value-based care models. Integration with artificial intelligence and telemedicine will likely accelerate, further smoothing the path from prescription to treatment. Meanwhile, hubs will continue to serve as the front line of coordination during public health emergencies, supply shortages and evolving insurance landscapes.
Ultimately, patient support hubs epitomize a shift towards patient-centric, coordinated care for complex therapies. Their architecture and data flows exemplify modern informatics solutions in healthcare, while their compliance frameworks demonstrate how innovation can be balanced with regulation. For stakeholders across the system – biopharma companies, providers, payers, and patients – understanding and optimizing hubs will remain a strategic imperative in the years ahead.
References
- Gannon Vanscoy, Continually Evolving Technology in Pharmacy Hub Services, Pharmacy Times, May 29, 2020 ([63]) ([5]).
- Gannon Vanscoy, Variations in The Specialty Pharmacy Hub Model, Pharmacy Times, June 16, 2020 ([25]) ([39]).
- Congressional Research Service, Legal Challenge to Patient Assistance Programs Puts Anti-Kickback Statute in the Spotlight, May 1 2025 (LSB11298) ([10]) ([11]).
- Council on Pharmacy Standards, Patient Onboarding & Consent Workflows (Module 10.3), 2024 ([8]) ([9]).
- Council on Pharmacy Standards, Patient Onboarding & Consent Workflows (Module 10.3), 2024 ([51]).
- Pharmaceutical Commerce, 2020 Patient Support / Hub Services Report, Nicholas Basta (Mar. 8, 2020) ([1]) ([15]).
- Pharmaceutical Commerce, 2020 Patient Support / Hub Services Report, Nicholas Basta ([22]) ([15]).
- Arijit Ganguli et al., The impact of patient support programs on adherence, clinical, humanistic, and economic outcomes: a targeted systematic review, Patient Preference and Adherence 10:711–725 (2016) ([12]).
- Case Study: Increasing Product Adoption Rate through EVERSANA’s Digital Hub Portal, Eversana (March 28, 2025) ([13]) ([14]).
- Surescripts Press Release, Specialty Patient Enrollment streamlines prescribing, (Sept. 2020) ([28]) ([64]).
- Surescripts Press Release, Transforms Prescribing Process for Specialty Medications Market, Sept. 2020 ([29]) ([54]).
- AvoidDropOff.com (phone support hub whitepaper), The Hub Model: A Centralized Approach to Maximize Patient Access (2011) ([4]) ([21]).
- Hopkin, Asembia (now part of Accredo), quoted in Improving Outcomes with Patient Support Services, Pharmaceutical Commerce, Feb. 2018 ([2]).
External Sources (64)

Need Expert Guidance on This Topic?
Let's discuss how IntuitionLabs can help you navigate the challenges covered in this article.
I'm Adrien Laurent, Founder & CEO of IntuitionLabs. With 25+ years of experience in enterprise software development, I specialize in creating custom AI solutions for the pharmaceutical and life science industries.
DISCLAIMER
The information contained in this document is provided for educational and informational purposes only. We make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability, or availability of the information contained herein. Any reliance you place on such information is strictly at your own risk. In no event will IntuitionLabs.ai or its representatives be liable for any loss or damage including without limitation, indirect or consequential loss or damage, or any loss or damage whatsoever arising from the use of information presented in this document. This document may contain content generated with the assistance of artificial intelligence technologies. AI-generated content may contain errors, omissions, or inaccuracies. Readers are advised to independently verify any critical information before acting upon it. All product names, logos, brands, trademarks, and registered trademarks mentioned in this document are the property of their respective owners. All company, product, and service names used in this document are for identification purposes only. Use of these names, logos, trademarks, and brands does not imply endorsement by the respective trademark holders. IntuitionLabs.ai is an AI software development company specializing in helping life-science companies implement and leverage artificial intelligence solutions. Founded in 2023 by Adrien Laurent and based in San Jose, California. This document does not constitute professional or legal advice. For specific guidance related to your business needs, please consult with appropriate qualified professionals.
Related Articles
Drug Formulary Tiers Explained: Step Therapy vs. PA Guide
Learn what drug formulary tiers are and how they affect prescription costs. Updated for 2026 with CMS-0057-F ePA rules, gold card laws, and IRA drug cost caps.
Value-Based Contracting in Pharma: Models & Challenges
An overview of value-based contracting (VBC) in pharmaceuticals, where drug prices are tied to patient outcomes. Covers models, challenges, case studies, CMS CGT Access Model (2025), finalized VBP rule (2026), and IRA drug price negotiations.
GLP-1 Market Access: PBM Prior Auth & First-Fill Metrics
Review 2026 GLP-1 market access metrics, including PBM prior authorization denial rates, turnaround times, and first-fill benchmarks for commercial teams.