
Veeva CTMS: Comprehensive Feature Overview for Clinical Trial Management
Veeva CTMS: Comprehensive Feature Overview for Clinical Trial Management
[Revised April 20, 2026]Veeva Clinical Trial Management System (CTMS) is an enterprise application from Veeva Systems designed to streamline and oversee all operational aspects of clinical trials. It serves as a single, cloud-based hub for managing studies end-to-end – from initial planning and site management through monitoring, issue resolution, and closeout – allowing clinical operations teams to "gain complete visibility across the portfolio" and unify trial information and processes for both insourced and outsourced studies ([1]) ([2]). By consolidating study data and workflows in one secure platform, Veeva CTMS helps sponsors and CROs execute trials faster and with higher quality, while maintaining compliance with global regulations ([3]). Below is an in-depth look at Veeva CTMS's features and how each module supports efficient, compliant clinical trial management.
Study Planning and Tracking
Veeva CTMS supports robust study planning and tracking capabilities that enable teams to proactively manage trial timelines and resources. Users can define and monitor key study milestones (e.g. site initiation, first patient in, database lock) across all trials – whether run in-house or outsourced – in a single system ([4]). The system provides tools to schedule and align operational activities with these milestones; for example, study planners can coordinate drug supply delivery with a planned site initiation visit to avoid delays ([4]). Milestones and trial events are tracked centrally, giving project managers an up-to-date view of progress and upcoming targets across the entire portfolio ([2]).
A critical aspect of planning is subject recruitment and enrollment forecasting. Veeva CTMS enables teams to plan the number of subjects to screen, enroll, and randomize at each level – study-wide, by country, and per site – and then track actual enrollment against these targets in real time ([5]). The system aggregates enrollment metrics from active sites (via direct EDC integration, discussed later) so that study teams can immediately see whether recruitment is on pace or lagging goals ([5]). Interactive dashboards display enrollment curves and screening metrics, updating automatically with incoming data, which allows early identification of enrollment bottlenecks and the ability to take corrective action (such as opening new sites or adjusting outreach) ([6]). By planning and tracking both operational milestones and patient enrollment in one place, Veeva CTMS helps organizations optimize trial timelines and adjust plans proactively to keep studies on schedule ([7]).
In addition, CTMS supports study calendar and visit schedule planning. Study managers can define protocol visit schedules and procedures within CTMS (e.g. how often visits occur, what assessments are done) to facilitate downstream scheduling and tracking ([8]). This seamless visit planning ensures that once the study is underway, expected subject visits and corresponding procedures are accounted for in the system's tracking, laying the groundwork for efficient monitoring and data collection.
Overall, the study planning and tracking module provides a strategic view for trial managers to plan resources and timelines across all ongoing studies. With a full global view of trial plans and real-time tracking of execution, CTMS enables more informed decision-making – teams can "actively manage activities, track key performance metrics, and mitigate delays in a unified system," leading to faster, more efficient trials ([9]).
Site Management and Investigator Management
Effective clinical trials require diligent site management and investigator relationship management, and Veeva CTMS provides a centralized solution to manage all site-related information and activities. At its core, CTMS serves as a global investigator and site repository, housing details on each trial site and principal investigator (PI) in one place ([10]). This includes site demographics and contacts, investigator credentials, site initiation and activation dates, enrollment numbers, monitoring visit history, and more. By consolidating this information, CTMS allows study teams to move away from disparate spreadsheets and maintain an accurate, up-to-date directory of all sites and investigators involved with the organization ([11]).
Within CTMS, users can log every interaction and communication with sites, building a complete history of the sponsor-site relationship. The system supports site communication logs to record calls, emails, and follow-ups, so that all team members have visibility into the latest site correspondence ([12]). Site managers can also document any resources assigned to the site (such as the CRA/monitor, site manager, or reading center), providing clarity on roles and responsibilities per site ([13]). This comprehensive view of site interactions helps strengthen collaboration with site staff and ensures no communication falls through the cracks.
Another key capability is tracking site status and performance across the trial lifecycle. CTMS captures each site's status (e.g. invited, initiated, active, on-hold, closed) and important dates (SIV date, first patient date, etc.), allowing real-time visibility into study startup and conduct at the site level ([4]) ([14]). Enrollment metrics are tracked per site, so the system can highlight underperforming sites – for instance, sites enrolling few or no patients can be quickly identified via reports ([7]). This enables data-driven decisions such as providing additional support to struggling sites or reallocating patients to higher-enrolling sites. By the same token, sites exceeding enrollment targets or performing well can be noted for future trials. Having this performance data readily available in CTMS allows clinical leaders to "assess site performance across studies" and take action to optimize trial execution ([15]).
Importantly, CTMS's site management is designed for global use and collaboration. Sponsors and contract research organizations (CROs) using CTMS can share site records and updates seamlessly. As one operations executive noted, "Veeva CTMS is the central hub of our trials, allowing study metrics and documents to flow seamlessly across our ecosystem… and improves how we work with CRO partners." ([16]). In practice, this means a sponsor can grant CRO team members appropriate access to the CTMS site records or leverage integration tools (like CTMS Transfer) to exchange site data, ensuring both parties are working from the same information. This unified approach reduces redundant data entry and keeps everyone aligned on site status and issues.
By empowering study teams with a complete view of site interactions and performance, Veeva CTMS improves site oversight and relationship management. Teams can collaboratively manage sites, strengthen investigator relationships through transparent communication, and make informed decisions on site support or corrective actions. Site management in CTMS ultimately contributes to improved study execution – when all site details are in one place, "we eliminate the need for disparate systems and manual data entry, reducing the risk of errors and ensuring data consistency across the entire study lifecycle." ([10]).
Monitoring and Visit Reports
Monitoring clinical sites is a core function of CTMS, and Veeva CTMS provides full support for planning, conducting, and documenting monitoring visits and trip reports. The system allows clinical research associates (CRAs) and monitoring teams to manage all types of monitoring visits – including pre-study visits (PSVs for site selection), site initiation visits (SIVs), interim monitoring visits (periodic routine visits), and close-out visits – in a structured workflow ([17]). For each site, monitors can schedule upcoming visits, generate confirmation letters and agendas, document the visit findings in a report, and issue follow-up letters or action items, all within the CTMS application ([18]). By standardizing the end-to-end monitoring process, CTMS ensures that no visit or required follow-up is missed and that visit documentation is thorough and compliant.
CRAs benefit from role-specific tools like the CRA Homepage in CTMS, which surfaces key information to prepare for visits. From a single dashboard, a CRA can view the current status of their assigned sites, recent enrollment numbers, open protocol deviations or other issues, and the last visit date ([19]). This role-based dashboard in CTMS helps the CRA prioritize which sites need attention and what to focus on during an upcoming visit (e.g. a site with lagging enrollment or many open queries) ([19]). With this unified view, "CRAs are better prepared to conduct initiation visits and follow-up activities… They can prioritize critical tasks, track enrollment status for each site, and review open issues… without leaving the system." ([19]). In other words, CTMS equips monitors with the context they need for efficient and targeted monitoring.
During monitoring visits, CTMS streamlines the authoring of visit reports (sometimes called trip reports). The system provides electronic visit report templates that can be filled out on-site or after the visit, replacing traditional paper forms or Word documents. Veeva CTMS's visit report module includes features like dynamic question branching, which automatically adjusts the report template based on prior answers or visit type ([20]). For example, if no investigational product is kept on site, sections related to drug accountability can be skipped. This automation speeds up report writing and ensures monitors address all relevant questions. According to Veeva, these efficiencies cut "time to author visit reports" by 50% on average ([21]) ([22]).
Once a monitoring visit report is completed in CTMS, the system can automatically file the report in the eTMF (electronic trial master file) for inspection readiness ([23]). Monitors no longer need to separately upload or email the report to the TMF team – CTMS and Veeva Vault eTMF are connected so that approved trip reports flow directly into the TMF repository with proper metadata ([23]). This not only saves time but also improves TMF completeness and compliance. In fact, one benefit of CTMS noted by users is that "when [study teams] author site visit reports, those reports automatically flow to eTMF", eliminating manual filing steps ([24]) ([23]).
CTMS also facilitates tracking of on-site findings and follow-ups. During or after a visit, a monitor can log any observations such as protocol deviations, regulatory non-compliance, data discrepancies, or action items for the site. These are captured in CTMS (often as part of the visit report or linked issue records) and can then initiate workflows for resolution (see Issue and Action Item Tracking below). The system can generate a follow-up letter summarizing required actions for the site, and this letter can be managed and tracked in CTMS to ensure the site responds and issues are resolved ([17]). All monitoring actions – scheduling, report completion, issue identification, letters – are recorded, providing a clear audit trail of site oversight in case of an audit ([25]).
Moreover, Veeva CTMS supports risk-based monitoring strategies through its risk assessment features. Study teams can define risk indicators and thresholds for their trials (for example, identifying sites with high query rates or poor compliance metrics) and use CTMS to capture and score these risks ([26]). This enables a risk-based approach where monitoring resources are focused on high-risk sites or processes. CTMS dashboards can highlight risk levels at the study, country, or site level, prompting the team to adjust the monitoring frequency or scope accordingly ([26]). By integrating risk assessment into CTMS, organizations align with the latest ICH E6(R3) guidelines on risk-based quality management, ensuring data quality is maintained efficiently. The E6(R3) guideline, finalized in January 2025, emphasizes Quality by Design (QbD) principles and proportionate oversight based on risk – approaches that CTMS directly supports through its risk-based monitoring and quality management capabilities ([26]).
In summary, the monitoring module of Veeva CTMS provides end-to-end support for the monitoring process: visit scheduling, preparation, report writing, and follow-up are all managed in one system. This not only boosts CRA productivity (with significant reductions in time and cost for monitoring reported ([27]) ([28])) but also improves oversight. Study managers can oversee monitoring progress and findings centrally, enabling them to take action sooner if a site is non-compliant or struggling. The result is more effective monitoring and ultimately higher quality trial conduct.
Issue and Action Item Tracking
During the course of a trial, various issues can arise – protocol deviations, regulatory non-compliance, data entry errors, safety signals, etc. Veeva CTMS includes robust issue and action item tracking functionality to ensure that all such problems are documented and resolved in a timely, controlled manner. This feature enables what Veeva describes as "closed-loop issue management," meaning every issue is logged, addressed with appropriate actions, and tracked to closure with full traceability ([29]).
When a deviation or issue is identified (for example, a missing consent form at a site, or a GCP non-compliance noted during monitoring), CTMS allows the user to capture the issue details in a dedicated form. The issue can be categorized (protocol deviation, quality issue, etc.), linked to the relevant study, site, and even specific visit or subject if applicable. Users can also record any immediate actions taken or attach supporting documentation. Once submitted, the issue record enters a workflow for review and resolution.
CTMS provides configurable workflows for issue resolution and follow-up actions. For instance, an issue can be automatically routed to a clinical operations manager or a quality assurance specialist for assessment. The responsible owner can then determine a corrective action or preventive action (CAPA) plan. Action items are logged in CTMS and tied to the issue – for example, the site might be tasked to retrain staff on a procedure, or a certain data point must be corrected in EDC. The system will track these action items, assign them to owners (with due dates), and send notifications as needed ([29]). Team members can easily see which issues are open and what steps are pending.
A major benefit is the ability to quickly identify and prioritize needed actions across all studies. The CTMS dashboards and reports can list all open issues and protocol deviations, along with their status and aging, giving trial managers a clear view of where intervention is required ([29]). By aggregating issues from all sites and studies, CTMS helps ensure that significant problems (e.g. a critical protocol deviation) get the necessary visibility and escalation. In fact, Veeva reports that using CTMS leads to "80% faster identification of issues" by study teams ([30]) ([31]), since the information is centralized and real-time. Additionally, built-in reports can analyze issue trends (for example, if multiple sites have the same issue, indicating a broader problem with the protocol or training), enabling proactive risk mitigation.
Each issue record in CTMS is maintained with a full audit trail of what was done and when, which is crucial for compliance. The system logs when the issue was opened, who was assigned, what actions were taken (and by whom), and when it was closed. This creates a complete compliance record demonstrating that the sponsor is following up on problems in accordance with GCP. CTMS also supports protocol deviation tracking as a specific subset of issue management, often required for compliance reporting. Monitors or site personnel can log protocol deviations in CTMS at the time of occurrence; these deviations can then be reviewed periodically (e.g. by a medical monitor or compliance committee) using CTMS reports ([32]). Veeva CTMS "simplifies regular protocol deviation reviews and action item management, enabling faster decision-making and keeping studies on track" ([32]).
By enforcing a consistent, transparent process for issue management, Veeva CTMS ensures that nothing falls through the cracks. Issues and their resolutions are documented in one place rather than scattered through emails or spreadsheets. Team members receive alerts for their action items, and managers can monitor the timeliness of issue closure. This not only improves operational efficiency but also strengthens compliance: regulators expect sponsors to actively manage trial issues, and CTMS provides the documentation to prove it. Ultimately, the issue and action tracking in CTMS contributes to higher data quality and patient safety – problems are identified sooner and resolved properly, preventing small issues from becoming larger risks. Sponsors using Veeva CTMS have found that it enables them to "proactively identify issues and take corrective action" before those issues threaten trial timelines or integrity ([7]).
Metrics and Reporting Dashboards
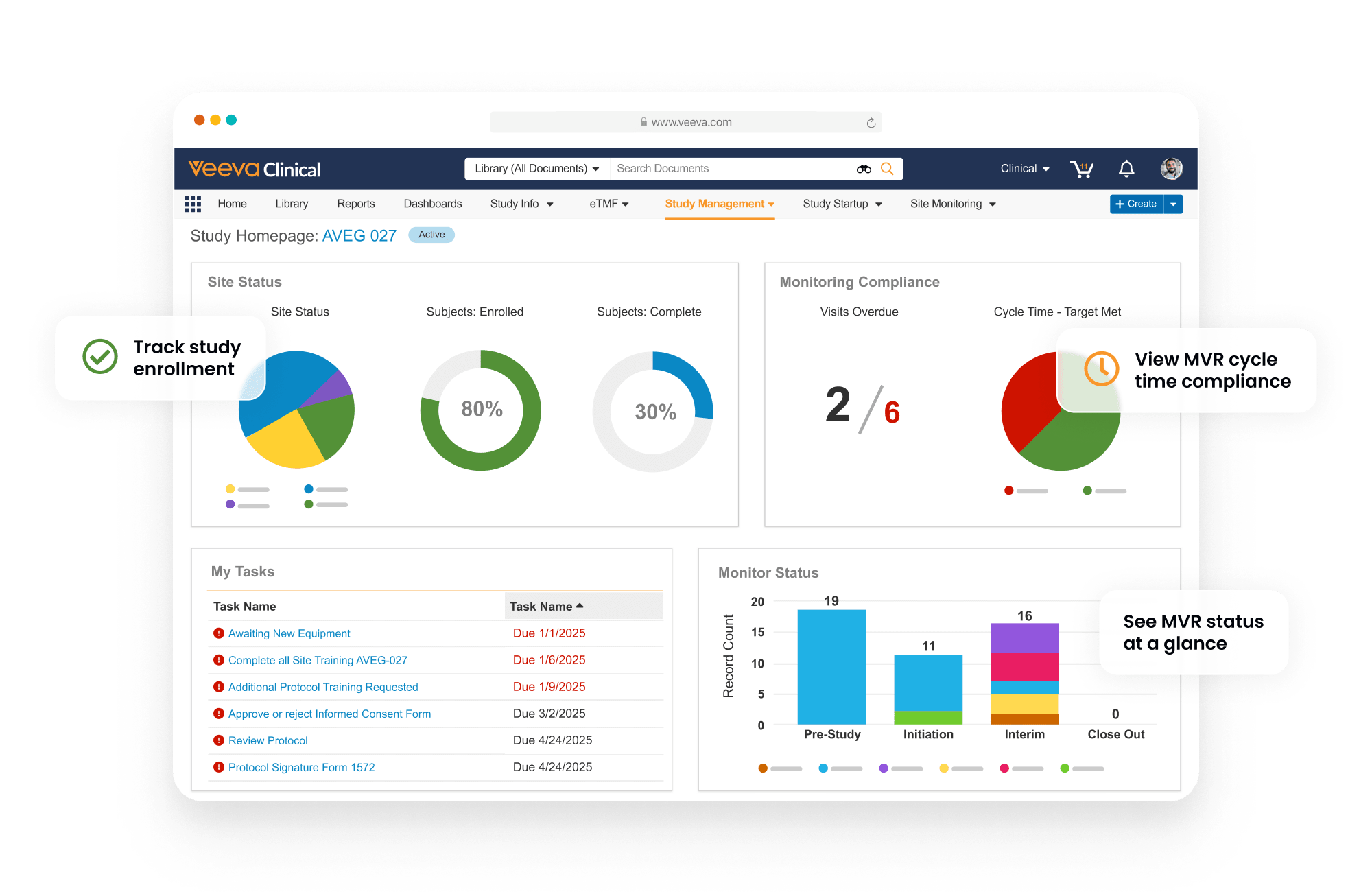
Veeva CTMS offers extensive reporting and dashboard capabilities, giving clinical operations teams real-time insight into study status, performance metrics, and operational bottlenecks. The system comes with out-of-the-box dashboards tailored for different roles (for example, a Study Manager dashboard and a CRA dashboard), and it also allows custom reports to be built for specific needs ([33]) ([34]). These dashboards aggregate data from across the CTMS – and connected systems like EDC – to present a live snapshot of trial progress at various levels.
Key performance indicators (KPIs) and metrics are tracked and visualized in CTMS dashboards. Users can monitor metrics by study, country, site, or even by study phase. Common metrics include: the number of sites initiated vs. planned, subject enrollment actual vs. target, subject visit compliance (missed visits, etc.), data entry timeliness, number of open queries or issues, protocol deviations, and monitoring visit status. For example, a Study Manager homepage might display a high-level status of all studies in the portfolio, highlighting enrollment progress and upcoming milestones for each ([33]). Drilling down, one could view a specific study's dashboard showing country-level enrollment, site activation counts, and the schedule of future monitoring visits.
One of the strengths of CTMS reporting is that the data is real-time and actionable. Because CTMS is connected to other systems and serves as the operational master, the moment a site is marked as initiated or a subject is enrolled (via EDC integration), that data reflects in the dashboards. Teams do not have to manually reconcile spreadsheets or wait for periodic reports – they have "real-time visibility into study progress, enrollment rates, and key performance indicators" at their fingertips ([35]). If a certain metric falls outside expected range (e.g. enrollment is 50% behind target this month), the CTMS dashboard will show that, and users can click through to investigate details (which sites are under-enrolling, etc.). Veeva highlights that interactive dashboards allow users to go "from insight to action", meaning you can navigate from a metric directly to the underlying records in CTMS and take remedial action ([36]). For instance, if a dashboard shows many open action items for a study, a user could click in to review and close those items within the same interface.
CTMS also provides a report builder for more customized or detailed reporting needs. Clinical operations teams can create reports that slice the data in various ways – by study phase, by indication, by site type (e.g. hospital vs clinic), etc. They can include data fields from CTMS like dates, status, and counts, and apply filters and grouping. For example, a user could build a report of "all protocol deviations in Phase II oncology studies in Europe" or "average time from site selection to activation per CRO-managed study". The interface is designed for business users (no coding required), and reports can be run on-demand or scheduled. These configurable reports help teams identify and resolve issues immediately by pinpointing where they occur ([37]) ([38]). Moreover, CTMS can export or share these reports if needed (for instance, generating a PDF for a governance meeting).
To facilitate focused oversight, the dashboards in Veeva CTMS are often role-based. Each functional role sees a dashboard with metrics relevant to their job. We mentioned the CRA view; similarly, a study project manager might see overall study health metrics, and an executive might see high-level portfolio metrics. These role-specific dashboards "provide real-time insights, enabling users to take action at the point of decision without logging in and out of multiple systems." ([37]) This is especially powerful in a unified platform like Veeva's – data from CTMS, eTMF, and other sources can be presented together. For example, a dashboard can combine study enrollment data with TMF document status to give a full picture of trial readiness. Users no longer need to juggle separate tools or spreadsheets; their CTMS dashboard becomes a one-stop shop for oversight.
In summary, the metrics and reporting capabilities of Veeva CTMS give clinical operations unprecedented real-time visibility and analytics for their trials. Teams can monitor progress continuously and respond to issues sooner (such as addressing a slow-enrolling site or deploying more monitors to a troubled region). Bottlenecks become apparent visually on the dashboard, which helps in eliminating operational bottlenecks and increasing efficiency ([36]). With data-driven insights readily available, organizations can make informed decisions to keep trials on track. This transparency and ability to course-correct quickly is a major factor in CTMS's value – it directly contributes to faster, more proactive trial management.
Regulatory and Compliance Support
Operating a clinical trial in a compliant manner is paramount, and Veeva CTMS is built with features to support regulatory compliance and adhere to guidelines like ICH GCP and 21 CFR Part 11 for electronic records. By centralizing trial information and processes, CTMS helps sponsors maintain the level of control and documentation that regulators expect. As Veeva notes, using CTMS allows companies to "maintain compliance with global regulations like ICH E6(R2) and (R3)" even as they accelerate execution ([3]).
ICH E6(R3) Update (2025): The final version of ICH E6(R3) Good Clinical Practice guidelines was published on January 6, 2025, representing a significant modernization of GCP standards. The European Medicines Agency announced an effective date of July 23, 2025, and the U.S. FDA published the final version in September 2025. ICH E6(R3) introduces a comprehensive risk-based quality management (RBQM) approach, promotes digital and decentralized trial methods, emphasizes quality by design with Critical to Quality (CtQ) factors, and provides expanded guidance on electronic systems including digital health technologies. Veeva CTMS's built-in risk management, electronic records capabilities, and audit trail features position organizations well to comply with these updated standards ([39]).
One way CTMS supports compliance is through comprehensive audit trails and electronic records management. Every action taken in the system (such as creating or updating a record, completing a workflow, or signing off a document) is time-stamped and recorded with the user's ID. These audit logs ensure traceability of who did what and when – a key requirement for regulatory inspections. Additionally, Veeva CTMS includes electronic signature capabilities for any regulated activities that require sign-off (for example, approving a monitoring visit report or formally confirming a protocol deviation assessment). The system's e-signatures are Part 11 compliant, with appropriate user authentication and signature manifestation (name, date, meaning of signature) captured for the record ([40]).
CTMS enforces role-based access controls to protect blinded information and maintain data confidentiality, another compliance aspect. Permission settings in CTMS ensure that users only see data appropriate for their role. For instance, a blinded study team member will not see treatment allocation information, and site personnel can be restricted from viewing other sites' data. These role-based access controls, along with audit trails and e-signatures, are built-in compliance features that ensure adherence to regulatory requirements and data integrity ([40]). They help demonstrate that the system is secure and trial data is reliable, which is crucial for regulatory audits.
Furthermore, by having one unified system, CTMS helps sponsors comply with the ICH E6 Good Clinical Practice directive on sponsor oversight. GCP requires sponsors to maintain oversight of CRO activities and ensure quality conduct of the trial. Veeva CTMS facilitates this by providing full visibility into CRO-managed tasks and centralizing all communications and documents. For example, CTMS's study oversight functionality allows sponsors to "track CRO activity and maintain communication logs to help ensure compliance with ICH/GCP guidelines." ([14]) All interactions with a CRO or investigator can be logged in CTMS, and any issues identified can be tracked to resolution, as described earlier. This means that if an inspector asks how the sponsor oversaw a trial, the CTMS can produce reports showing the frequency of monitoring visits, the issues found and fixed, and correspondence with sites – fulfilling the sponsor's GCP obligations.
In terms of regulatory document tracking, while a dedicated eTMF system is typically the system of record for regulatory submissions and trial master file documents, CTMS does intersect by tracking expected documents and regulatory milestones. Veeva CTMS can be configured with expected document lists per milestone (for example, expecting IRB approval letters, regulatory green light, etc., before a site initiation). It can then flag if any required document is missing for a site. This feature, when used in conjunction with Vault eTMF, ensures that all essential documents are in place to meet regulatory requirements before progressing to the next step (like activating a site). By integrating with eTMF, CTMS helps maintain an "inspection-ready" state for trials, since operational data in CTMS aligns with documents in the eTMF ([23]).
Additionally, CTMS supports compliance with regulatory timelines and commitments. For instance, if a certain safety report must be filed to authorities within 15 days, CTMS can track that timeline as a milestone or action item. The workflow engine can send reminders or escalate if the deadline is approaching. All these controls reduce the risk of non-compliance due to oversight or human error.
Finally, the validation status of Veeva CTMS as a cloud system is worth noting. Veeva performs rigorous validation of its software and provides validation documentation to customers, which helps companies use CTMS in a validated state (a requirement for systems managing GxP data). The platform is updated regularly (three times a year with new releases) under a controlled change process, and customers can choose to adopt new functionality as needed while staying compliant. This ensures that using Veeva CTMS does not compromise a company's regulatory compliance stance; on the contrary, it often strengthens it by providing a well-controlled digital environment.
In summary, Veeva CTMS was designed with compliance in mind: it centralizes trial data in a controlled, auditable environment so that sponsors can confidently meet regulatory requirements. With CTMS, organizations can more easily enforce GCP standards, manage protocol adherence, and generate the necessary documentation to pass audits. Compliance is no longer a separate burden but a natural output of using the system – as data and processes are handled in CTMS, "built-in features like audit trails, electronic signatures, and role-based controls ensure regulatory adherence and data integrity." ([40]) This allows study teams to focus on trial execution knowing that compliance is being systematically managed in the background.
Integration with Other Clinical Systems (eTMF, EDC, etc.)
Modern clinical trial operations rely on multiple specialized systems, and one of Veeva CTMS's strengths is its ability to integrate with other clinical systems to enable an end-to-end information flow. In particular, CTMS is tightly integrated with electronic data capture (EDC) and electronic trial master file (eTMF) systems – including Veeva's own offerings – to eliminate duplicate data entry and ensure that all stakeholders are working with consistent, up-to-date data.
EDC Integration: Veeva CTMS can connect directly with EDC systems to exchange key trial data in real time. For example, Veeva CTMS is "connected with Veeva EDC to support enrollment, monitoring, payments, and navigation to casebooks directly from within CTMS." ([21]) In practice, this means that as subjects are enrolled or visit data is entered in the EDC, that information can flow into CTMS without manual intervention. Enrollment numbers and visit statuses are updated in CTMS automatically, powering the real-time recruitment dashboards and allowing monitors to see the latest EDC data (like critical datapoint deviations or missing forms) when planning site visits. Conversely, study and site information managed in CTMS (like new site records or updates to study milestones) can be pushed to the EDC to keep both systems in sync ([41]). Veeva provides a standard Clinical Operations <> EDC connection for its Vault CDMS (EDC) product, where "Studies, Study Countries, and Sites" defined in CTMS can be transferred to the EDC, and "Subjects, Subject Visits, Procedures, and Visit Definitions" from EDC are sent to CTMS ([41]). This ensures that CTMS and EDC share a common data model and trial definitions, reducing reconciliation work. Even if a sponsor uses a third-party EDC, Veeva CTMS's open API and integration tools allow similar data exchange, so that CTMS remains the up-to-date repository of enrollment and visit status.
eTMF Integration: As noted earlier, Veeva CTMS also connects with eTMF systems (such as Veeva's Vault eTMF) to ensure trial documentation and operational data remain aligned. The integration is exemplified by the automatic transfer of monitoring visit reports and confirmation/follow-up letters from CTMS to eTMF upon finalization ([23]). Additionally, CTMS can send other records (e.g., protocol deviations logged in CTMS could generate a document or reference in the TMF, or site progress reports from CTMS could be archived in TMF if needed). The integration means that the TMF is always populated with the latest artifacts from trial conduct managed in CTMS, supporting inspection readiness. It also works in reverse for certain cases: for instance, if a document required for a milestone is filed in eTMF, CTMS could be updated (or at least referenced) to reflect that the requirement is met. By linking CTMS and eTMF, Veeva enables a single source of truth across operational data and documents – trial information only needs to be entered once and can be leveraged across systems ([42]). This not only saves time but also prevents errors that come from inconsistent data in separate systems.
Other Integrations: Veeva CTMS's integration capabilities extend to other clinical and enterprise systems as well. The platform can integrate with safety systems (to share serious adverse event information, for example), with clinical data warehouses or BI tools (to feed CTMS data into broader analytics), and even with investigator grant/payment systems. In the Veeva ecosystem, Vault CTMS is part of the Veeva Clinical Operations platform, so it natively connects with other Vault applications like Study Startup, Payments, and Site Connect. For instance, Vault Payments (a separate module) can be used alongside CTMS to manage site payments: CTMS will feed it enrollment and monitoring visit data needed for payment triggers ([43]). Similarly, CTMS <-> Study Startup integration means that as sites are activated in the Study Startup system, that status is reflected in CTMS.
One notable integration feature specific to Veeva is CTMS Transfer for CRO collaboration. Many sponsors use CROs who may have their own CTMS or own Vault. Veeva CTMS offers a capability called CTMS Transfer that "automates the daily transfer of data between sponsors and CROs using Veeva CTMS" ([44]). Essentially, if both the sponsor and CRO are on Veeva CTMS (even in separate vaults), CTMS Transfer can synchronize study and site data, monitoring visit dates, subject enrollment, and other information on a scheduled basis ([45]). This ensures both parties have an identical view of trial status without manual reconciliation. It greatly improves sponsor-CRO collaboration and oversight, as the sponsor can see CRO-entered updates in near real time. CTMS Transfer was introduced as a new innovation to facilitate "greater visibility" for sponsors over outsourced trials ([46]).
New in 2025: Veeva SiteVault CTMS for Research Sites. In April 2025, Veeva announced Veeva SiteVault CTMS, a clinical trial management system designed specifically for research sites. This new offering integrates with SiteVault eISF and SiteVault eConsent to allow sites to comprehensively manage clinical trials within one unified system. Key features include bidirectional data flow with sponsors using Veeva's Clinical Platform, study visit scheduling and procedure tracking, invoice generation and payment tracking, and seamless sharing of study team roles and participant information across eISF and CTMS. SiteVault CTMS is free for sites managing up to 20 concurrent active studies (covering over 90% of research sites), with the initial release in August 2025. Over 450 sponsors already use Veeva to connect with 10,000+ study sites, and this new site-focused CTMS further strengthens the sponsor-site digital ecosystem ([47]).
The net effect of these integrations is that Veeva CTMS acts as a unified hub in the clinical IT landscape. Instead of operating CTMS in isolation, sponsors can connect it to their other systems so that data flows freely and accurately. For users, this is a major advantage – they no longer need to log into multiple applications and re-enter or export/import data. "A unified platform that easily connects with other clinical systems eliminates costly integrations and facilitates seamless data exchange," which is a key trait of a modern CTMS ([48]). It means that when a project manager opens CTMS, they can trust the data (e.g. enrollment figures, site status) to be current, because it's automatically updated from the source systems. Likewise, downstream systems (like TMF) receive inputs from CTMS without extra effort. This tight interoperability not only improves efficiency but also reduces errors and ensures that everyone – clinical operations, data management, site management, etc. – is working from the same consistent data. In summary, Veeva CTMS's integration capabilities allow it to support end-to-end trial management across system boundaries, truly making it the "central hub of trials" that connects people, data, and processes in one ecosystem ([16]).
Role-Based User Access and Workflows
Veeva CTMS is designed to accommodate the various roles involved in clinical trials, from CRAs and study managers to project directors and beyond. It features a comprehensive role-based user access model and configurable workflows that together ensure each user has the appropriate permissions and task assignments. This combination of fine-grained access control with tailored workflows is critical for maintaining both security and efficiency in trial operations.
Role-Based Access Control: In CTMS, every user is assigned one or more roles (e.g., CRA/Monitor, Study Manager, Data Manager, Clinical Research Coordinator, etc.), and each role is associated with specific permissions and data access rules. This ensures that users see and do only what they are supposed to. For example, a CRA role might allow editing of monitoring reports and creation of trip reports for assigned sites, but might not allow editing core study milestones or viewing financial information. A study project manager role, on the other hand, could have access to edit study-level planning data and view aggregated metrics, but perhaps not see blinded subject data. By configuring roles to match organizational responsibilities, CTMS helps maintain blinding and data confidentiality (as required in many trials) and protects sensitive information while still enabling users to do their jobs. The system's role-based controls are even considered part of its compliance framework, as they help enforce that only authorized personnel perform certain actions ([40]).
Moreover, role-based access in Veeva CTMS ties into the user experience: dashboards and views are often role-specific. We discussed how CRAs have a specialized homepage showing site-specific metrics, while Study Managers have a broader study overview. These are driven by the user's role. The navigation and available tabs in CTMS can also be configured per role – e.g., a CRA might have quick links to "My Sites" and "My Visits" whereas a Lead might have links to "All Studies" and "CRO Oversight." This customization improves usability and helps users focus on relevant tasks. It also reduces training effort since each role's interface can be simplified. The LinkedIn guide on CTMS emphasizes a "user-friendly interface that facilitates easy navigation, reducing the learning curve and increasing user adoption" ([49]), which is aided by tailoring what each role interacts with.
Configurable Workflows: Beyond static role permissions, Veeva CTMS includes a powerful workflow engine that automates multi-step processes and routes tasks to the right users/roles. Many activities in clinical operations follow standard processes – for example, reviewing a monitoring visit report typically involves the CRA drafting it, a CTM or project manager reviewing it, and maybe a QA person giving final approval. CTMS can automate this process: once the CRA completes the report and clicks submit, the system will automatically assign a task to the designated reviewer (based on role or a specific person for that study). The reviewer gets notified (via email or notification in CTMS) and can approve or reject the report. If rejected, it can route back to the CRA for updates; if approved, the workflow ends and triggers the next step (like auto-filing to eTMF). This kind of streamlined, automated workflow is configurable for many processes – site initiation approvals, protocol amendment rollout, issue escalation, etc. – according to each organization's SOPs ([50]).
By implementing workflows in CTMS, organizations ensure standardization of trial processes and reduce manual coordination. The system effectively orchestrates tasks across different roles: "streamlined workflows and automated processes ensure efficient and accurate capture, tracking, and updating of study details, reducing manual effort and minimizing errors." ([51]) For instance, consider protocol deviation handling: CTMS can be set so that when a CRA logs a protocol deviation, a workflow automatically notifies the clinical study lead and creates a task for them to assess the deviation. The lead can document the assessment and mark if a corrective action is needed, which could then trigger an assignment to the site manager to follow up. All participants get alerts when it's their turn to act, and CTMS tracks the state of each workflow step. This replaces back-and-forth emails or phone calls, ensuring a more reliable process. Nothing gets lost because CTMS keeps the item open until all required steps are completed and the issue is closed.
Workflows in CTMS are highly configurable to match different trial needs. Admin users can often adjust workflow steps, notifications, and roles involved without programming, using the Vault platform's configuration tools. This allows adaptation to company-specific processes or regulatory requirements. For example, if a company's SOP requires quality assurance sign-off on all monitoring visit reports within 15 days, the CTMS workflow can incorporate a QA approval step and even send reminder notifications if the 15-day window is nearing expiry.
Another aspect of automation in workflows is notifications and alerts. CTMS can automatically send email notifications or system alerts to users when certain events occur or if deadlines are missed. For instance, if a site's planned initiation date passes without the site being activated in the system, CTMS could alert the study lead. Or if a certain report is pending approval for over a week, it could notify a supervisor. These automated nudges help keep the trial on track without a coordinator manually checking everything.
In summary, role-based access and workflows in Veeva CTMS work hand-in-hand to drive efficient collaboration. The role permissions make sure each user has the right level of access and sees an interface optimized for their responsibilities. The workflows then tie those roles together in end-to-end processes, automatically handing off tasks and information to the correct person at the correct time. This not only improves productivity (less time spent figuring out who needs to do what, or chasing people for updates) but also ensures compliance with defined processes. As the LinkedIn article notes, Veeva CTMS's advanced workflow management "ensures that study details are accurately captured, tracked, and updated in real-time, minimizing errors and fostering transparency across all stakeholders." ([52]) Everyone knows their tasks via CTMS and can trust that once they do their part, the system will route the next step appropriately. In a complex trial with many moving parts, such clear workflow orchestration is invaluable.
Global Collaboration Tools
Clinical trials today are global endeavors, often involving stakeholders spread across sponsors, CROs, and investigator sites around the world. Veeva CTMS is inherently a cloud platform, which means all authorized users can access it from anywhere, anytime, providing a foundation for global collaboration. In addition, it offers specific collaboration tools and features that help study teams work together more effectively across geographic and organizational boundaries.
One fundamental collaborative aspect is the single, shared data environment that CTMS provides. All team members – whether at the sponsor or a CRO partner – working on a study can be given access to the same CTMS vault (with appropriate role-based permissions as discussed). This eliminates the problem of each party maintaining their own trackers and then reconciling later. When a sponsor outsources trial management to a CRO, they can still log into CTMS and see up-to-date status, because the CRO is recording progress directly in the sponsor's CTMS. Conversely, if the CRO uses their own CTMS, the CTMS Transfer feature can sync data to the sponsor. In both cases, everyone is literally on the same page, which drives efficient collaboration. The press release from Inhibrx highlighted that using a connected CTMS "saves time and effort for our lean team and improves how we work with CRO partners." ([16]). This is because both sponsor and CRO share metrics and status through CTMS rather than via weekly reports or spreadsheets.
Beyond data sharing, Veeva CTMS has built-in capabilities for document and information sharing among study team members. For instance, CTMS allows users to upload attachments to various records (like attaching a regulatory approval PDF to a site record). Team members with access to that record can then retrieve the document without having to email it around. CTMS also supports a commenting or discussion feature on records, so users can leave notes or tag other users for input. This facilitates conversations in context (e.g., a project manager can tag a CRA in an issue record asking for an update) rather than siloed email threads.
Another collaboration tool is the integration of CTMS with Veeva's Site Connect and SiteVault for site-side interactions (though SiteVault is technically a separate product, we'll stay high-level). Essentially, Veeva is enabling a direct digital link between the sponsor's CTMS and the site's systems so that things like document exchange (sending safety letters, etc.) can happen within the platform. While not a core CTMS feature per se, CTMS works in concert with these tools to streamline sponsor-site communication. For example, CTMS can trigger sending of a new version of the Investigator Brochure to sites via Site Connect, and track that it was acknowledged. This kind of automated information sharing cuts down on email and ensures sites get what they need promptly ([13]).
On a day-to-day level, Veeva CTMS aids collaboration through task assignments and notifications. Team members can assign tasks to one another within CTMS (as part of workflows or as ad-hoc tasks), and the assignees are notified and can update the task status. This is particularly useful for geographically dispersed teams – a manager in the US can assign a task to a monitor in Europe at the end of their day, and the monitor in Europe sees it at the start of theirs, working asynchronously but efficiently. The system maintains the context and history of the task, so even across time zones the purpose and status of work is clear.
Veeva CTMS's global usability is also enhanced by its multi-language support. The Vault platform (and thus CTMS) is available in many languages, allowing users in different countries to use the interface in their preferred language ([53]). Dates and formats can also adapt to locales. This reduces barriers for local teams and site-facing personnel, fostering wider adoption. Everyone still interacts with the same underlying data, but in a language comfortable to them, which is a subtle but important factor in global collaboration.
Because CTMS is cloud-based and accessible anywhere, it supports remote and decentralized trial models as well. Especially in recent times with travel restrictions or the rise of remote monitoring, CTMS enables teams to continue collaborating without physical presence. Monitors can perform remote visit assessments in CTMS, and site staff can update status through integrated systems, all of which the sponsor can see in real time.
To illustrate the collaborative benefits, the LinkedIn case study on CTMS noted: "With Veeva CTMS, we have a global site directory that houses all our information. We can see what sites and principal investigators we've worked with without relying on spreadsheets." ([11]). This quote underscores how having a centralized, globally accessible repository (for site info in this case) replaces the need for each region or partner maintaining their own lists. It strengthens institutional knowledge and avoids duplicate work. Another point from that study is the ability to "seamlessly collaborate with study team members" as one of the outcomes of a real-time, unified CTMS ([7]).
Additionally, CTMS provides tools for coordination meetings and oversight. For example, during weekly study team calls, teams can pull up the CTMS dashboard and collectively review the latest metrics, rather than each person quoting different numbers. The data consistency enhances trust and communication among the team. If questions arise (like "why is site X behind?"), the answers can often be found directly in CTMS (in site notes or issue logs), again keeping the discussion anchored in one system.
In summary, Veeva CTMS facilitates global collaboration by providing common platforms, shared data, and integrated tools for all stakeholders. It breaks down silos between sponsors and CROs, connects central teams with local site monitors, and provides transparency across regions. Features like communication logs, document sharing, and in-system notifications further enhance teamwork by making CTMS not just a database, but an interactive workspace for the trial. As a result, study teams can work in a more coordinated fashion, leading to fewer miscommunications and faster issue resolution. In the words of one industry professional, the powerful features of CTMS "enhance collaboration and ensure regulatory compliance, ultimately driving the success of our clinical trials." ([54]) Global collaboration isn't just about videoconferences and emails – it's about having the right shared system, and CTMS provides exactly that for clinical operations.
Automation and Workflow Engine
Automation is a key element of Veeva CTMS's value proposition – by automating repetitive or complex tasks, CTMS frees up clinical operations staff to focus on critical decision-making and oversight. We have touched on many automated aspects (like workflows and data integrations) in earlier sections. Here, we'll summarize how CTMS's automation and workflow engine works to streamline trial management.
At its core, Veeva CTMS is built on the Veeva Vault Platform, which includes a powerful workflow and rules engine. This engine allows the configuration of custom business rules and triggers based on events in the system. For example, CTMS can be configured such that when a certain milestone is reached (like a site is activated), the system automatically triggers creation of the next set of expected activities (like scheduling the site's interim monitoring visits). This goes beyond basic workflows – it's about using defined logic to have the system carry out steps that otherwise would be done manually by a coordinator.
A prominent automated feature in CTMS is the dynamic forms for visit reports and other templates. As noted, the monitoring visit report form uses dynamic branching logic ([20]). This is essentially automation embedded in the user interface – the form automatically adjusts itself to fit the context (a kind of decision-tree logic built in), meaning CRAs don't need to manually skip irrelevant sections. This reduces human error (forgetting to fill something out that should be filled, or wasting time on not applicable sections) and ensures consistency in report completion.
CTMS's integration features also count as automation: the CTMS-to-EDC and CTMS-to-eTMF data flows are automated via system jobs or real-time APIs, so that no person has to manually transfer data between these systems. The CTMS Transfer between sponsor and CRO vaults, for instance, runs as an automated daily job moving the latest data over ([45]). This kind of automation greatly reduces latency in information sharing; a sponsor gets yesterday's updates from the CRO by the next morning without anyone sending a file. It also eliminates errors that can creep in with manual data transcription. Essentially, wherever data can be synced or tasks can be systematized, Veeva CTMS attempts to automate that process.
Another area of automation is notifications and reminders, which we alluded to. CTMS can auto-send notifications for pending approvals, approaching deadlines, or delayed milestones. For example, if a monitoring visit report has been sitting with a reviewer for over X days, CTMS can send a reminder email. Likewise, upcoming site re-monitoring due dates can trigger reminders to schedule the visit. These automated nudges ensure that trial activities keep moving according to plan, acting as a safety net against human forgetfulness.
CTMS also automates various status calculations and roll-ups. Enrollment percentages, site activation rates, study progress bars – these are calculated by the system in real time based on raw data, rather than an analyst having to compute them. Risk scores in the risk-based monitoring module are calculated from input factors automatically ([26]). Even things like protocol deviation tallies per site are auto-counted. This not only saves time but provides immediate feedback. For instance, if one site has a spike in deviations, CTMS will show that count in dashboards without anyone needing to compile it.
Vault CTMS's workflow engine is flexible enough to automate complex multi-step processes. For example, a site closure process might involve 1) CRA marks last visit done, 2) CTMS automatically checks that all queries are resolved (via EDC data), 3) CTMS then creates a task for document reconciliation in eTMF, 4) once completed, CTMS updates site status to closed and notifies the study lead. Such a sequence can be automated with minimal human intervention besides the decisions and checks themselves. This ensures processes are consistent across studies and sites.
An additional benefit of automation is speed and efficiency gains. By reducing manual administrative work, CTMS helps cut overall trial management effort. Veeva's data shows significant reductions in monitoring effort and other areas due to CTMS automation ([27]) ([22]). For example, if CTMS reduces the time a CRA spends on paperwork by automating report filing and follow-ups, that CRA can devote more time to site engagement or additional sites. Automation also contributes to faster study startup and closeout, as tasks happen in parallel or immediately when criteria are met. This is one way CTMS helps accelerate study execution on the whole.
From a technical perspective, administrators can extend CTMS automation via Vault's configuration. They can create custom triggers (called object lifecycles and actions in Vault) that respond to data changes. For instance, a custom rule could automatically populate a field or send a notification if a certain combination of data appears (like a high severity issue at a high-enrolling site might trigger an alert to a quality director). This level of customization ensures CTMS can adapt to evolving needs and continue automating new scenarios as processes change or new regulatory requirements come in.
To summarize, the automation capabilities of Veeva CTMS cover everything from routine data transfers to sophisticated workflow orchestration. The system was designed to minimize manual effort for trial management: "streamline processes and automate tasks" is a core theme ([52]). Users of CTMS benefit from these automations by experiencing fewer administrative delays, getting real-time updates without manual work, and having the confidence that the system is automatically ensuring things happen when they should. Automation in CTMS not only improves efficiency but also reduces variability – every study follows the set processes reliably. This leads to more predictable outcomes and the ability to manage more trials with the same resources, a crucial advantage in today's fast-paced clinical trial environment.
Data Standards and Real-Time Visibility
Veeva CTMS is built around the principle of a single source of truth, which inherently promotes consistent data standards and real-time visibility into trial data. By using CTMS as the authoritative system for clinical operational data (and integrating it with other systems as discussed), organizations can enforce uniform data definitions and access up-to-the-minute information at all times.
Unified Data Model: Veeva's Vault Clinical platform, which includes CTMS, uses a unified data model for studies, countries, sites, etc. This means that all applications in the suite share common definitions for these objects. For CTMS users, this ensures that everyone is speaking the same language in terms of data. There is one master list of study IDs and site codes, one set of country names, one definition of what constitutes a protocol deviation, and so on. Having this single, centralized repository for all study-related information (protocol details, site info, patient enrollment, regulatory data, etc.) enforces data standards across the organization ([10]). It reduces the risk of discrepancies that often occur when different teams maintain their own spreadsheets (where, for instance, a site might be referenced by slightly different names in two places). In CTMS, data fields are defined globally and used consistently, improving clarity and integrity of information.
Master Data Management and Standards: Veeva CTMS effectively acts as a master data management tool for clinical trial operations. Trial attributes like phase, therapeutic area, indication, and region can be standardized in CTMS picklists. This allows consistent categorization of studies and sites, which is essential for cross-study reporting and regulatory submissions. For example, when pulling metrics across studies, you can trust that "Phase 2" means the same thing in all records because the data is standardized in CTMS. If using industry standards (like CDISC definitions for trial phases or endpoints), those can be configured into CTMS as well. CTMS also maintains data lineage – because it is the system of record for operational data, any changes (like an update in a site address or a correction in enrollment count) are logged and the current correct value is always clear.
Crucially, Veeva CTMS provides real-time visibility into the data it holds. Since CTMS is cloud-based and typically updated continuously (either by users entering data or by integrations bringing in new data), the information visible on CTMS dashboards and reports is as current as possible. There is no need to wait for end-of-week summaries or manual consolidation. For example, if a patient was enrolled this morning at a site, by afternoon the CTMS enrollment dashboard and the site's enrollment count will reflect that new patient (assuming an integration or quick user entry). This immediacy is what sponsors mean by having real-time oversight. It enables truly proactive management – catching issues as they happen rather than weeks later. Lack of real-time visibility was cited as a major challenge with legacy processes ([55]), and CTMS addresses that by giving an up-to-date window into trial operations.
Another aspect of real-time visibility is the ability for all stakeholders to see the same data simultaneously. In CTMS, if a CRA updates a site status, the study manager and anyone else with access can see that update immediately. There's no version confusion or email lag. This transparency ensures decisions are made on the latest facts. Teams can even use CTMS in real-time meetings or reviews (for instance, screen-sharing a CTMS dashboard in a meeting to jointly examine current progress). It fosters a culture of data-driven decision-making.
By having standardized data and real-time updates, CTMS also improves data quality. Errors or outliers in data can be spotted quickly when the data is consistently structured and timely. For example, if one site reports an impossibly high screening number, CTMS dashboards might flag it for review (as it stands out against standardized metrics). Additionally, because CTMS pulls data from sources like EDC directly, it avoids transcription errors. Manual data entry points are reduced, hence fewer opportunities for typos or misalignment. Veeva notes that "unifying trial documents and operational data in a single system improves accuracy" and enables better planning ([56]). When data is accurate and current, teams can trust the system and forego time-consuming validations or cross-checks that they would do if they doubted the data.
In terms of data standards compliance, Veeva CTMS supports compliance with standards like ICH E6(R3) (finalized in January 2025, which emphasizes Quality by Design, risk-based quality management, and proportionate oversight) by providing the tools to implement those standards (like risk-based monitoring, issue management). For 21 CFR Part 11, CTMS's audit trails and e-signatures ensure that the electronic data is trustworthy, which is a standard in itself for electronic records. While these are regulatory standards, they dovetail with data integrity principles often referred to as ALCOA (Attributable, Legible, Contemporaneous, Original, Accurate) – CTMS facilitates meeting all of those for trial data.
Another benefit of using CTMS as the central system is during regulatory inspections or internal audits: when asked to provide data on study status or a history of an issue, the CTMS can generate an authoritative report with timestamps and owner info that is standardized. This is much more straightforward than cobbling together files from different regions or teams.
Finally, CTMS's real-time data and standardized structure set the stage for advanced analytics and AI. With all operational data in one place, companies can apply data analytics tools to predict timelines or identify risk patterns. Because the data is uniform, such analyses are more reliable. Veeva itself delivers enhanced analysis and insights through its dashboards ([36]).
Veeva AI (2025-2026): Veeva announced plans for Veeva AI Agents across all Veeva applications, with availability starting December 2025 for commercial applications and expanding across R&D and quality in 2026. These AI agents are built into the Veeva Vault Platform and designed for specific, high-impact use cases. They understand the application context, have application-specific prompts and safeguards, and have direct, secure access to Veeva application data, documents, and workflows. Veeva AI uses large language models (LLMs) from Anthropic and Amazon, hosted on Amazon Bedrock. Customers can also configure and extend Veeva-delivered AI Agents and build their own custom agents. For clinical operations specifically, Veeva AI is expected to enhance document generation (including informed consent forms), supercharge TMF bots to automatically extract fields and QC documents, and deliver significant cost and efficiency improvements. Many companies are now using a mix of rule-driven and AI-based automation after successful pilot programs in 2024-2025 ([57]).
In conclusion, data standards and real-time visibility in Veeva CTMS go hand in hand to ensure that clinical trial data is consistent, reliable, and instantly available to those who need it. By serving as the single source of truth for operational trial data, CTMS eliminates the fragmentation and delays that hinder decision-making in clinical operations. As a result, study teams can rely on CTMS to provide a "real-time visibility into study progress, enrollment rates, and KPIs, enabling proactive decision-making and timely interventions." ([35]) This high-fidelity view of trial operations is a cornerstone of running faster, quality trials with confidence in the data.
Mobile Capabilities
In today's fast-paced environment, having access to trial information on the go is highly valuable. Veeva CTMS, being part of the cloud-based Vault platform, offers mobile capabilities that allow clinical operations professionals to stay connected to their studies via smartphones or tablets. Through the Veeva Vault Mobile app, users can securely log into CTMS from iOS or Android devices and perform many key actions anywhere, anytime ([58]) ([59]).
With Vault Mobile, CTMS users can view and update records on the move. For example, a CRA traveling between investigator site visits can pull up the app to review the latest enrollment numbers or check if any urgent issues were reported at a site. They can navigate through their studies, countries, and sites just like on the desktop, but with an interface optimized for mobile. This ensures that even when away from their computer, users have real-time dashboards and reports at their fingertips – the app lets you "see real-time dashboards" for study metrics on a mobile screen ([60]). This could be very useful in meetings or while multitasking, providing up-to-date insights without needing a laptop.
The mobile app also supports completing tasks and approvals. Users can receive push notifications on their device when a CTMS task is assigned to them (for instance, a monitoring report to approve or an issue to review) ([61]). They can then open the task in the app, review the relevant information, and complete the task (approve/reject, etc.) on the spot. This responsiveness can speed up processes significantly – a manager could approve a site activation while out of office, or a medical monitor could sign off on a deviation assessment from home, avoiding delays. The app even allows certain document-related tasks like viewing and commenting on documents, which ties into CTMS if, say, an attached file needs review ([62]).
For monitors and field personnel, mobile access is particularly beneficial. They can use a tablet during site visits to input notes or update CTMS in real time (assuming internet connectivity). While Vault Mobile currently requires an internet connection to function (it's not offline-enabled) ([63]), Wi-Fi or cellular networks are usually available in most locations. Monitors might use a tablet to fill out a visit report template in CTMS directly during the visit. This not only saves time later, but ensures data is entered contemporaneously. Even if they don't complete the full report on site, they could at least log key observations or mark the visit as done, which immediately notifies others in the team that the visit took place.
Another aspect of mobile utility is for site-facing roles or regional personnel who might not be at a desk regularly. For example, a site liaison or a regional trial lead can quickly pull up CTMS on their phone to answer questions like "How many patients have been enrolled at Site X?" or "Is that document fully signed off yet?" without needing to boot a laptop. This kind of agility can improve communication with investigators and stakeholders by providing answers on the spot.
The Vault Mobile app is continuously improving (it gets updated with each triannual Vault release) and supports all Vault applications, meaning a CTMS user can also potentially access related eTMF documents or study startup info if their role permits, all from the same app ([64]). It supports all the same languages as the web app, ensuring a global workforce can use it comfortably ([53]).
Security is, of course, a major consideration. The Vault mobile app uses the same secure authentication as the web (it can integrate with single sign-on, etc.), and no data is stored permanently on the device. If a device is lost, administrators can revoke access. This means mobile access does not compromise the secure environment required for clinical data – data is viewed and edited in real time but not kept on the device, and the app does not collect any personal data itself ([65]).
In summary, mobile capabilities in Veeva CTMS extend the power of the system beyond the office, increasing the flexibility for users. Whether it's a project manager checking a dashboard on an iPad in a meeting or a CRA completing tasks on her phone at the airport, the ability to "access your Vaults on the go" and "find and view documents, complete tasks, [and] see real-time dashboards" is a significant advantage ([59]). It ensures that critical trial information and actions are never out of reach, which can accelerate decision-making and keep trials moving smoothly. This mobile support aligns with the modern expectation that enterprise software should be available whenever and wherever needed – and in the context of clinical trials, it helps teams remain responsive and informed at all times.
Recent Developments: SiteVault CTMS and Veeva CTMS Basics
Veeva continues to expand its CTMS ecosystem with significant announcements in 2025. In April 2025, Veeva announced Veeva SiteVault CTMS, a clinical trial management system specifically designed for research sites. Released in August 2025, SiteVault CTMS is integrated with SiteVault eISF and SiteVault eConsent, allowing sites to comprehensively manage clinical trials within one main system.
A key feature of SiteVault CTMS is its bidirectional data flow with sponsors using Veeva's Clinical Platform. This integration enables seamless data exchange between sites and sponsors, reducing manual processes and increasing efficiency. According to Nick Frenzer, General Manager of Site Solutions at Veeva, "High-quality cloud software and seamless sponsor integration will help sites be more efficient."
Notably, SiteVault CTMS is free for sites managing up to 20 concurrent active studies, which represents over 90% of research sites. This initiative reflects Veeva's commitment as a Public Benefit Corporation to improve clinical research accessibility for sites of all sizes. Sites can upgrade to SiteVault Enterprise for larger operations without requiring specialized training or professional services to maintain the system.
Additionally, in May 2025, Veeva announced that its Veeva Basics platform is now utilized by more than 75 biotech companies. The new Veeva CTMS Basics application provides an accessible entry point for smaller organizations to leverage CTMS capabilities for improved efficiency and reduced costs in clinical operations.
Conclusion: End-to-End Oversight for Faster, Quality Trials
Veeva CTMS, with all the features described above, provides an end-to-end solution for clinical trial management that empowers clinical operations teams to oversee trials holistically, act faster, and ensure high quality and compliance. By centralizing study planning, site management, monitoring, issue resolution, and reporting in one platform, CTMS gives sponsors and CROs complete real-time oversight of their trials from start to finish. Every module – whether tracking a milestone or logging an issue – feeds into the larger picture of trial progress, enabling informed, proactive management decisions.
This comprehensive system has a direct impact on study execution speed. Manual steps are eliminated or automated (for example, no more duplicating data entry across systems, or chasing paper reports), which reduces administrative burden and saves time. Workflow automation accelerates processes like report reviews and site approvals that traditionally slow down trials. With CTMS, teams can identify bottlenecks early (be it a lagging site or a document delay) and address them before they impact timelines, thereby "optimizing trial execution" and keeping studies on schedule ([9]). In fact, organizations using Veeva CTMS have reported significant efficiency gains – for instance, a reduction of monitoring costs by 30% and faster completion of visit reports ([27]) ([22]) – which translates to faster trial completion or the ability to handle more trials in parallel.
At the same time, CTMS improves data quality and consistency across trials. With a single source of truth and standardized workflows, the data captured is more accurate and errors are caught and corrected promptly. The integrated issue management and risk management capabilities ensure that quality issues are not only documented but also resolved in a timely manner, leading to cleaner data. The system's design inherently promotes compliance with good clinical practice, which in turn means the trial data is credible. One VP of operations noted that after implementing Veeva CTMS to bring trial management in-house, they wanted "real-time access to our data" to avoid losing oversight, and CTMS provided that visibility and control ([11]). Real-time data access means any anomalies can be scrutinized immediately, and trends (like site performance or data entry lag) can be analyzed to make course corrections that improve overall data integrity.
Crucially, Veeva CTMS helps ensure regulatory compliance is upheld throughout the trial. By centralizing operational data and documents and providing audit trails and controlled workflows, CTMS makes it easier to comply with regulations and to demonstrate that compliance. Sponsors can confidently show auditors that they maintained oversight, followed approved processes, kept secure records, and managed issues according to regulation. As mentioned, CTMS supports compliance with ICH GCP E6(R3) guidelines (finalized January 2025) on oversight and quality, as well as electronic records requirements. Companies using CTMS can thus accelerate their trials "while maintaining compliance with global regulations" ([3]), achieving both speed and quality – a combination that is often hard to balance.
Another intangible but important benefit is enhanced team collaboration and transparency, which we discussed. When all stakeholders collaborate in one system, it fosters a culture of accountability and openness. Everyone can see what is going on (according to their role), which builds trust and ensures that responsibilities are clear. This collaborative environment, supported by CTMS, leads to faster problem-solving and a unified approach to trial management, as opposed to siloed teams each with partial information.
In conclusion, Veeva CTMS stands out as a modern, comprehensive CTMS platform that supports end-to-end clinical trial oversight. It accelerates study execution through process automation and real-time tracking, improves data quality by enforcing consistent management and rapid issue resolution, and ensures regulatory compliance with built-in controls and a complete audit trail ([40]) ([3]). All these capabilities are delivered in a single cloud system that is flexible and scalable to an organization's needs. As of January 2025, more than 200 companies – including 17 of the top 20 biopharmas – have adopted Veeva CTMS for these reasons, replacing legacy systems and spreadsheets with this unified solution ([66]) ([16]). By leveraging Veeva CTMS, clinical operations professionals can manage trials with greater efficiency, insight, and confidence, ultimately bringing therapies to patients faster and with robust documentation of how they did it. The platform's technical strengths and user-focused design make it a powerful engine driving modern trial management practices toward better outcomes for all stakeholders.
Sources:
-
Veeva Systems – Vault CTMS Features Overview ([42])
-
Veeva Systems – Better Trials, Better Outcomes: Why Every Biopharma Needs a CTMS ([37]) ([19])
-
Veeva Systems – Better Trials, Better Outcomes: Why Every Biopharma Needs a CTMS ([32]) ([36])
-
Veeva Systems – Press Release: More Than 200 Companies Advance Trial Management with Veeva CTMS ([16]) ([3])
-
K. Jeyapal (LinkedIn) – Veeva Vault CTMS for Study Details – Key Features ([10]) ([40])
-
K. Jeyapal (LinkedIn) – Veeva Vault CTMS for Study Details – Key Features ([51]) ([54])
-
Veeva Systems – Vault Help Documentation (CTMS & EDC Integration) ([41])
-
Veeva Systems – Vault Help Documentation (CRA & Study Manager Dashboards) ([33]) ([70])
-
Veeva Systems – Apple App Store – Veeva Vault Mobile App Description ([59])
-
FDA – ICH E6(R3) Good Clinical Practice Guidelines ([39])
-
Veeva Systems – Veeva Announces Research Site Clinical Trial Management System ([47])
-
Veeva Systems – Announcing Veeva AI ([57])
External Sources (70)

Need Expert Guidance on This Topic?
Let's discuss how IntuitionLabs can help you navigate the challenges covered in this article.
I'm Adrien Laurent, Founder & CEO of IntuitionLabs. With 25+ years of experience in enterprise software development, I specialize in creating custom AI solutions for the pharmaceutical and life science industries.
DISCLAIMER
The information contained in this document is provided for educational and informational purposes only. We make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability, or availability of the information contained herein. Any reliance you place on such information is strictly at your own risk. In no event will IntuitionLabs.ai or its representatives be liable for any loss or damage including without limitation, indirect or consequential loss or damage, or any loss or damage whatsoever arising from the use of information presented in this document. This document may contain content generated with the assistance of artificial intelligence technologies. AI-generated content may contain errors, omissions, or inaccuracies. Readers are advised to independently verify any critical information before acting upon it. All product names, logos, brands, trademarks, and registered trademarks mentioned in this document are the property of their respective owners. All company, product, and service names used in this document are for identification purposes only. Use of these names, logos, trademarks, and brands does not imply endorsement by the respective trademark holders. IntuitionLabs.ai is an AI software development company specializing in helping life-science companies implement and leverage artificial intelligence solutions. Founded in 2023 by Adrien Laurent and based in San Jose, California. This document does not constitute professional or legal advice. For specific guidance related to your business needs, please consult with appropriate qualified professionals.
Related Articles
Medidata CTMS and EDC: Comprehensive Clinical Software Analysis
Explore Medidata Rave CTMS and EDC solutions, including their history, features, and real-world application in clinical trials. Learn about market standing and competitors.

SAP in the Pharmaceutical Industry: Enterprise Solutions for Drug Development and Manufacturing
A comprehensive analysis of how pharmaceutical companies leverage SAP's enterprise solutions for drug development, clinical trials, manufacturing, supply chain management, and regulatory compliance, with detailed case studies from leading pharma companies.

Why Veeva Split from Salesforce: Pharma CRM Shake-Up
A comprehensive analysis of Veeva's decision to end its partnership with Salesforce, exploring the strategic implications, timeline of events, and impact on life sciences companies facing this major industry transition.